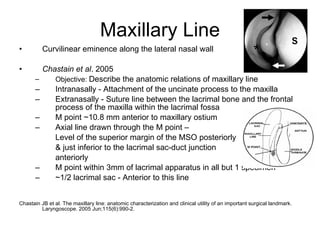
The document discusses the anatomy and etiology of acquired nasolacrimal duct obstruction. It describes the normal anatomy of the lacrimal drainage system and locations of the nasolacrimal duct. It also discusses common causes of acquired nasolacrimal duct obstruction including congenital factors and discusses evaluations including lacrimal pump function and Shirmer testing to differentiate types of epiphora. Sex and age can affect the size of the bony nasolacrimal canal.