03/20/2025 1
Emergency DepartmentVersus Urgent
Care Patient Flow
Maximizing Patient Throughput and Addressing
Patient Satisfaction
ER
ED
Urgent Care
2.
03/20/2025 2
Where doyou go if you really
really feel horrible?
• Two Main Options:
– Urgent Care
– Emergency Room
– Can anyone tell me the difference?
3.
03/20/2025 3
Urgent Care
•Urgent care is not emergency
care. Urgent care centers are same-
day clinics that can handle a
variety of medical problems that
need to be treated right away, but
are not considered true
emergencies.
• Urgent cares are often equipped
with X-ray, lab and other diagnostic
services, and as a result can handle
4.
03/20/2025 4
Urgent Care
•Symptoms that can be evaluated
and treated at an urgent care clinic
include:
• Fever without a rash
• Vomiting or persistent diarrhea
• Abdominal pain
• Wheezing or shortness of breath
• Dehydration
• Moderate flu-like symptoms
5.
03/20/2025 5
Urgent Care
•“Many people use the emergency
room as a place to receive after-
hours care for minor illnesses or
injuries without realizing they have
another option,” says Dr. Evans.
6.
03/20/2025 6
Emergency Room
•Hospital emergency departments
provide medical care at any time,
day or night. Unlike urgent care
centers or walk-in clinics, they are
equipped and staffed to handle the
most complex or critical needs,
including life- and limb-threatening
situations ranging from heart
attack and stroke to traumatic
injuries following a car accident
7.
03/20/2025 7
Emergency Room
•Symptoms that are best evaluated in an
emergency room include:
• Broken bones and dislocated joints
• Fever with a rash
• Seizures
• Severe cuts that may require stitches
• Facial lacerations
• Severe cold or flu symptoms
• Bleeding with pregnancy
8.
03/20/2025 8
Emergency Room
•Symptoms that are best evaluated in an
emergency room include:
• Chest pain or difficulty breathing (SOB)
• Weakness/numbness on one side
• Slurred speech
• Fainting/change in mental state
• Serious burns
• Head or eye injury
• Concussion/confusion
9.
03/20/2025 9
Where doyou go?
• Talk with your classmate and make a
decision:
• Scenario 1:
• Patient complains of headache after
drinking too much?
10.
03/20/2025 10
Where doyou go?
• Talk with your classmate and make a
decision:
• Scenario 2:
• You fell off your scooter, but you feel ok,
just a minor sratch?
11.
03/20/2025 11
Where doyou go?
• Talk with your classmate and make a
decision:
• Scenario 3:
• You think you are having a heart attack
12.
03/20/2025 12
Where doyou go?
• Talk with your classmate and make a
decision:
• Scenario 4:
• You feel like you have the flu but don’t
have time to see your family (regular
doctor).
13.
03/20/2025 13
Where doyou go?
• Talk with your classmate and make a
decision:
• Create your own:
• 1 for Urgent Care
• 1 for Emergency Room
Emergency Medicine
Healthcare Environment
•Hospital Operating Paradigms
– Decreased National Capacity
– Late discharges
– Keep patients “out”
• Primary Care Physician Availability
– MD’s are at capacity
– No after hours care
• Patient population
– Elderly and Complexity
• Insurance
– Underinsured
– EMTALA
• Hospital Capacity
– Beds reduced ---Demand increased
– Excess capacity was surge capacity
– 15% required for efficiency
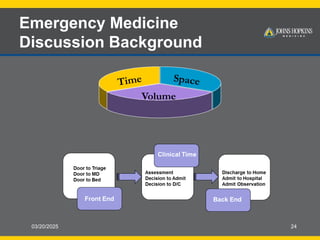
Time Space
Volume
17.
Emergency Medicine
Service Expectations
•24 Hour Service
• Minimal Waiting Time
• Demand Based Service
• Different Expectations AND A Different Standard
– It’s okay to wait days for my MD but not hours in ED
• Convenience and Episodic Care
Drive thru if possible!!!
18.
18
Emergency Medicine
Quality PatientCare
• Quality Indicator
– Service
• Time
– Communication
• Amount and Type of
communication
– Clinical Quality
• Outcomes
• Quality Measure
– Wait time
– Throughput times
– Walkout Rate
– Satisfaction Surveys
– Compliance with practice
standards
• STEMI
• Sepsis
• Pneumonia
• Trauma
– Adverse Events
03/20/2025 20
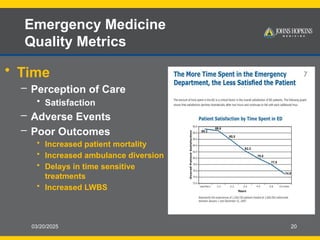
Emergency Medicine
QualityMetrics
• Time
– Perception of Care
• Satisfaction
– Adverse Events
– Poor Outcomes
• Increased patient mortality
• Increased ambulance diversion
• Delays in time sensitive
treatments
• Increased LWBS
21.
Emergency Medicine
All aboutProcess
Moderate Acuity
Level 3
Segmenting Patient Flow in the ED
Med/Surg
Dx and Rx
Likely Discharge
Complex medical
Dx and Rx
Possible Admission
Main ED
Clinical Decision Unit
Process Time
22.
03/20/2025 22
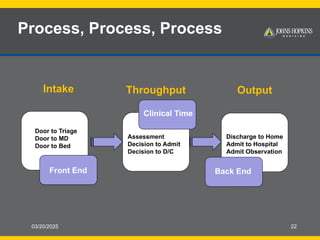
Process, Process,Process
Intake Throughput Output
Door to Triage
Door to MD
Door to Bed
Front End
Clinical Time
Assessment
Decision to Admit
Decision to D/C
Discharge to Home
Admit to Hospital
Admit Observation
Back End
23.
03/20/2025 23
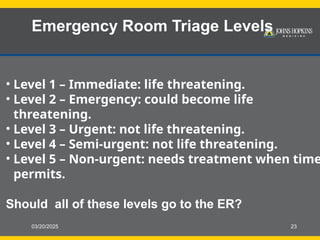
Emergency RoomTriage Levels
• Level 1 – Immediate: life threatening.
• Level 2 – Emergency: could become life
threatening.
• Level 3 – Urgent: not life threatening.
• Level 4 – Semi-urgent: not life threatening.
• Level 5 – Non-urgent: needs treatment when time
permits.
Should all of these levels go to the ER?
03/20/2025 25
Discussion and
Questions
•Best Practices: Front, Middle, Back End
• Related Questions:
– What are the most important metrics to use in order to
monitor success?
– As a way of managing “excess” volume, are there
hospitals who successfully redirect patients to alternate
treatment sites?
– Who in your system is responsible for the care of the
patient who is boarding in the ED?
– Has anyone identified an effective way to manage
physician practice variability?
26.
03/20/2025 26
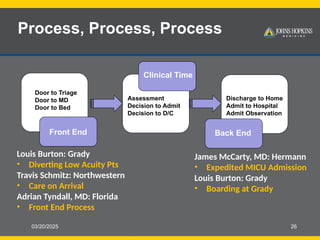
Process, Process,Process
Door to Triage
Door to MD
Door to Bed
Front End
Clinical Time
Assessment
Decision to Admit
Decision to D/C
Discharge to Home
Admit to Hospital
Admit Observation
Back End
Louis Burton: Grady
• Diverting Low Acuity Pts
Travis Schmitz: Northwestern
• Care on Arrival
Adrian Tyndall, MD: Florida
• Front End Process
James McCarty, MD: Hermann
• Expedited MICU Admission
Louis Burton: Grady
• Boarding at Grady
27.
03/20/2025 27
Strange ERCases
• Impromptu Presentations:
• Spend 5 minutes researching the
weirdest/strangest more wasteful
cases in the ER. This can be in any
country.
• Then your group will spend 2-3
minutes telling us about the case.
• WWWWWH
• OREO




































![mark [Autosaved].ppt](https://cdn.slidesharecdn.com/ss_thumbnails/markautosaved-231014033343-789ae37c-thumbnail.jpg?width=640&height=640&fit=bounds)






![mark [Autosaved].ppt](https://cdn.slidesharecdn.com/ss_thumbnails/markautosaved-230818103222-21644599-thumbnail.jpg?width=640&height=640&fit=bounds)
























