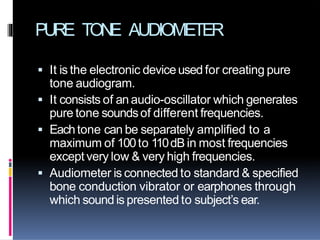
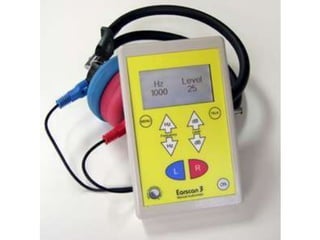
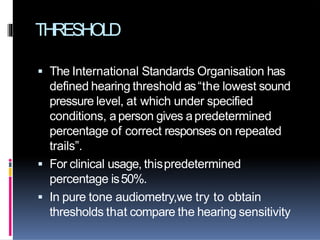
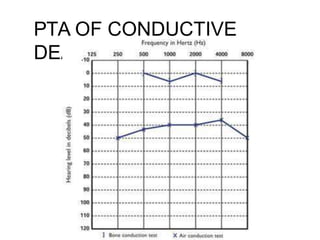
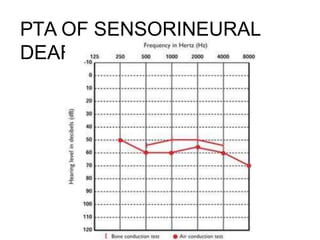
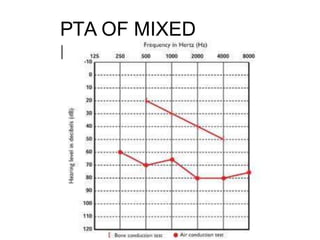
Pure tone audiometry is used to test hearing sensitivity to pure tones. It can determine if a subject has a hearing loss and what type by comparing air and bone conduction thresholds. The audiometer generates pure tones of different frequencies that are presented through headphones or a bone vibrator. Threshold is the lowest sound level at which a subject responds correctly 50% of the time. Interpreting the pure tone audiogram can indicate if a hearing loss is conductive, sensorineural, or mixed based on the air-bone gap and differences in thresholds.


![DECIBEL & OTHER
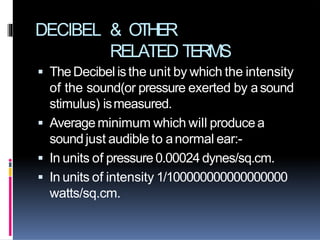
RELATED TERMS
BEL-Aratio expressedin logarithm(with base
10)which tells ushow many times the sound
we are measuring is stronger or weaker than
areferencesound.(0-14)
[BEL=log IO/IR]
DECIBEL-one tenth ofBEL.
[DECIBEL(dB)=10 logIO/IR]
SPL-signifies that apressure reference has
been used(i.e. referencesound has apressure
level of .00024dynes/sq.cm.)](https://image.slidesharecdn.com/puretoneaudiometry-200422132217/85/Pure-Tone-Audiometry-10-320.jpg)

























































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
