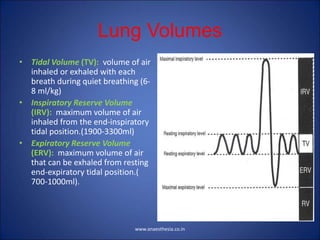
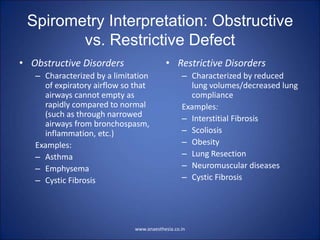
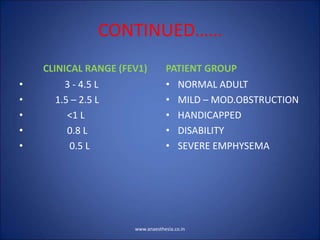
Pulmonary function tests measure lung volumes and capacities through tracings. There are four lung volumes - tidal volume, inspiratory reserve volume, expiratory reserve volume, and residual volume. Five lung capacities are measured by adding up different lung volumes - inspiratory capacity, expiratory capacity, vital capacity, functional residual capacity, and total lung capacity. Pulmonary function tests provide objective measurements of lung function to assess respiratory dysfunction and its severity. Common tests include measuring vital capacity, inspiratory capacity, expiratory capacity, and functional residual capacity.






















































![Spirometry Pre and Post Bronchodilator
• Obtain a flow-volume loop.
• Administer a bronchodilator.
• Obtain the flow-volume loop again a minimum of 15
minutes after administration of the bronchodilator.
• Calculate percent change (FEV1 most commonly
used---so % change FEV 1= [(FEV1 Post-FEV1
Pre)/FEV1 Pre] X 100).
• Reversibility is with 12% or greater change.
www.anaesthesia.co.in](https://image.slidesharecdn.com/14-240326051217-aa9c235b/85/Pulmonary-Function-Tests-and-it-s-importance-ppt-75-320.jpg)
























![THYROID DISORDERS AND ANAESTHESIA.ppt[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/thyroiddisordersandanaesthesia-240826093351-632c8bba-thumbnail.jpg?width=640&height=640&fit=bounds)























































