- An echocardiogram 6 weeks to 3 months after valve implantation allows assessment of surgery results and serves as a baseline.
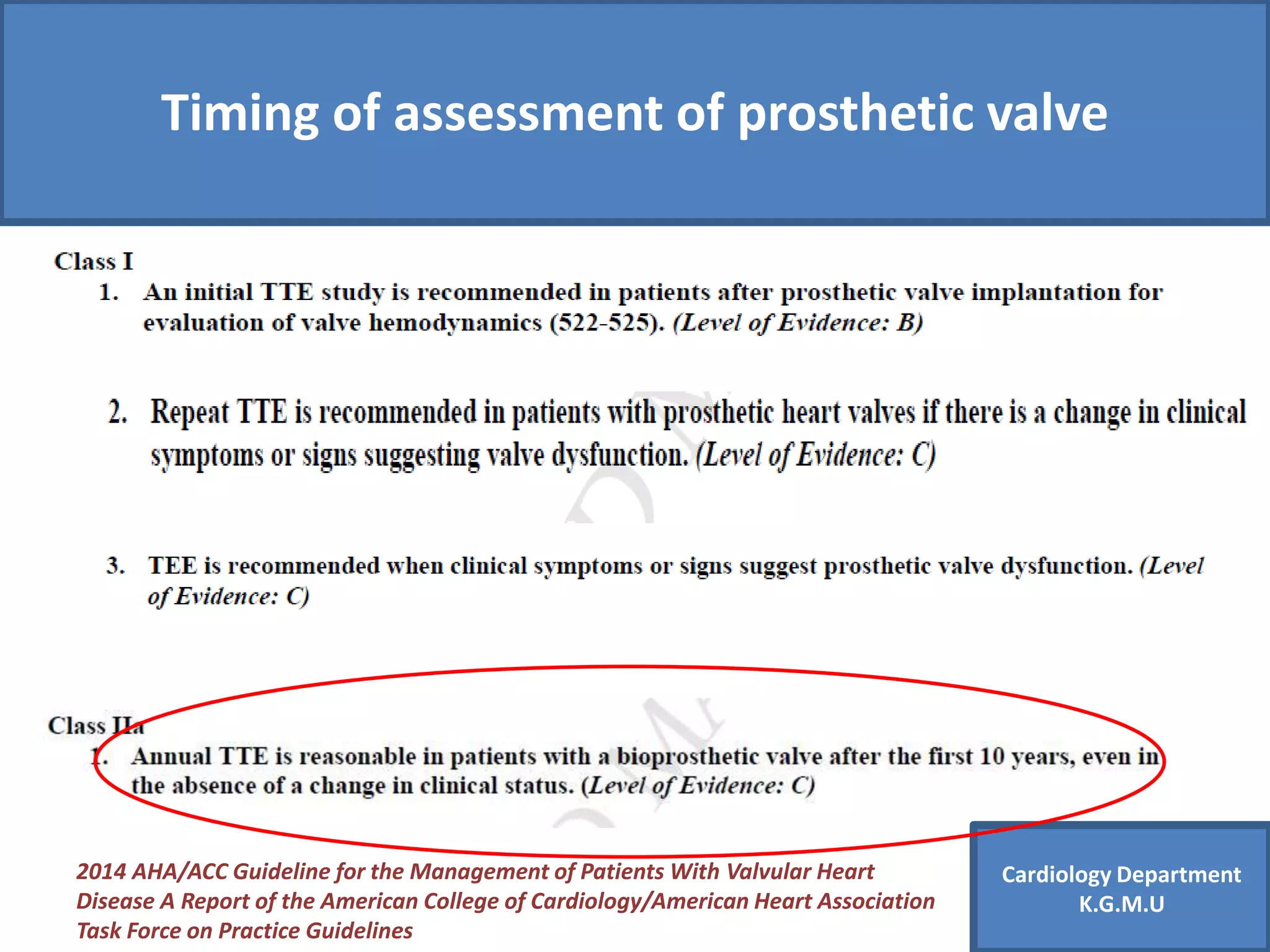
- Asymptomatic patients with mechanical valves usually need annual exams unless complications arise.
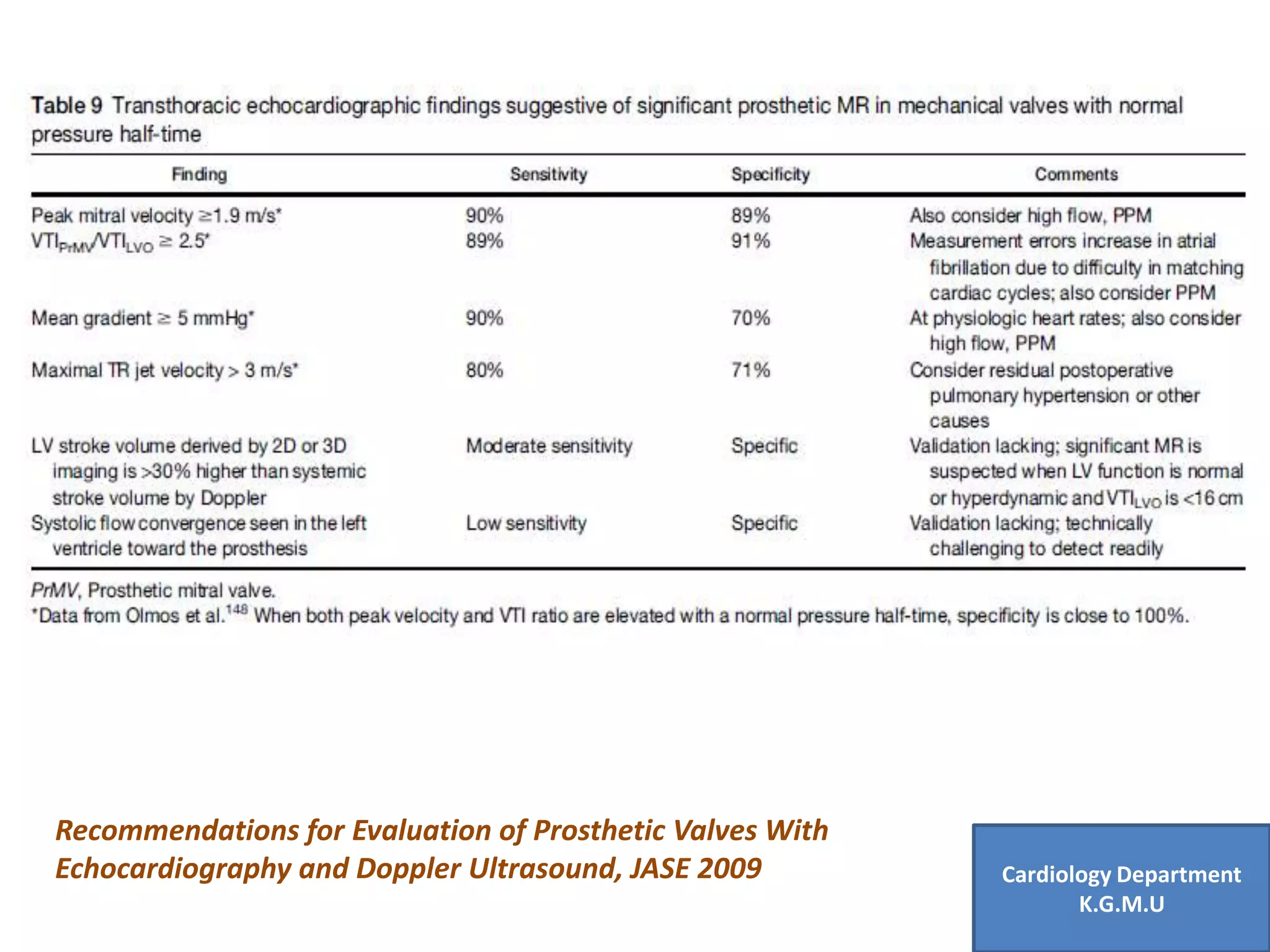
- Echocardiograms evaluate leaflet motion, pannus/thrombus formation, gradients, and regurgitation to assess prosthetic function.
- Doppler indices like DVI help determine stenosis while features like mobile echoes indicate pannus or thrombus.