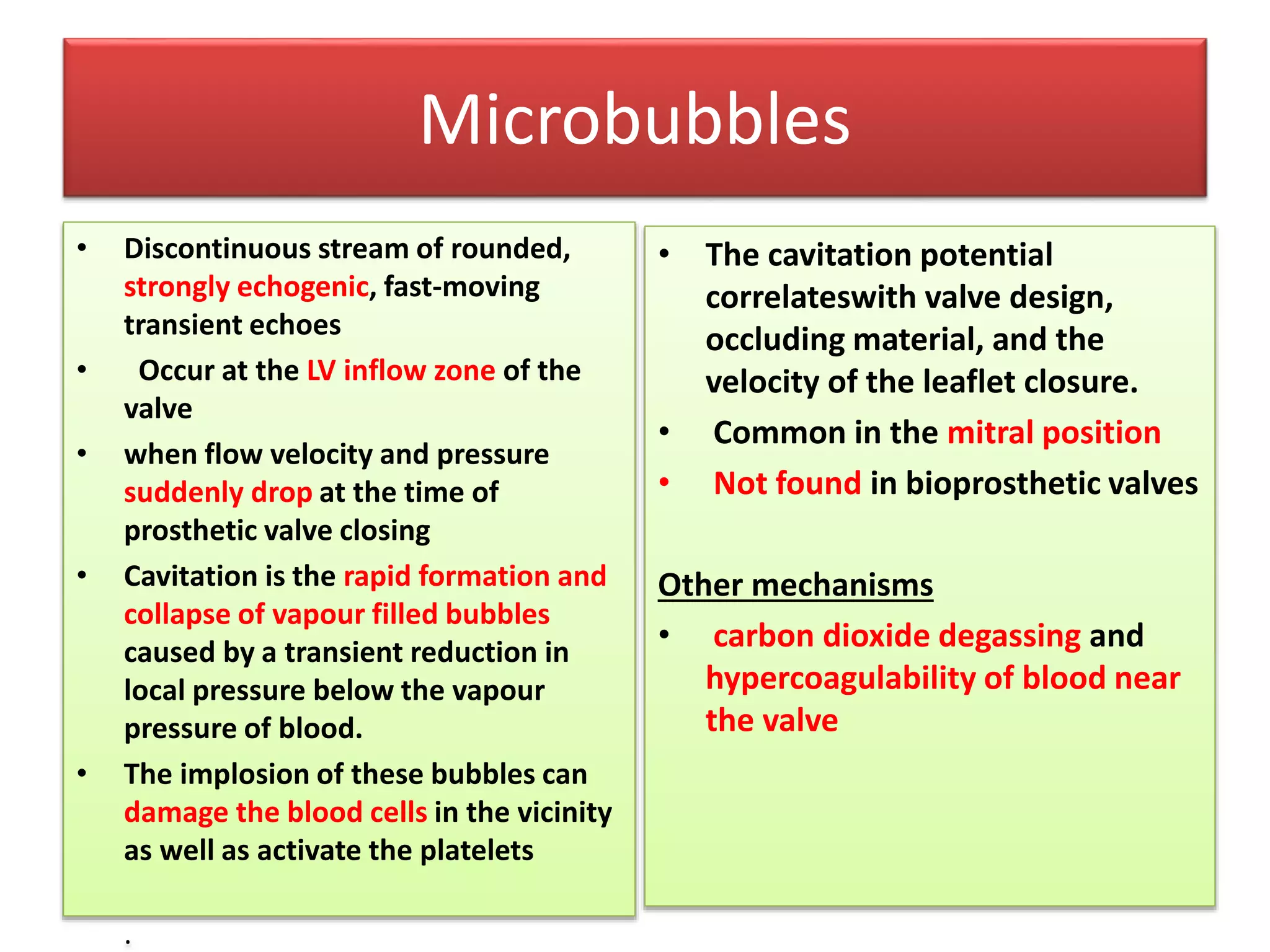
This document discusses echocardiographic assessment of prosthetic heart valves. It provides guidance on timing follow-up echocardiography after valve replacement surgery and assessing valve function and complications. Key goals of Doppler interrogation include evaluating obstruction or regurgitation of prosthetic valves. Effective orifice area, velocity indices, and pressure gradients help quantify stenosis. Color flow imaging aids in grading paravalvular leaks or regurgitation. Microbubbles and strands may indicate valve dysfunction.