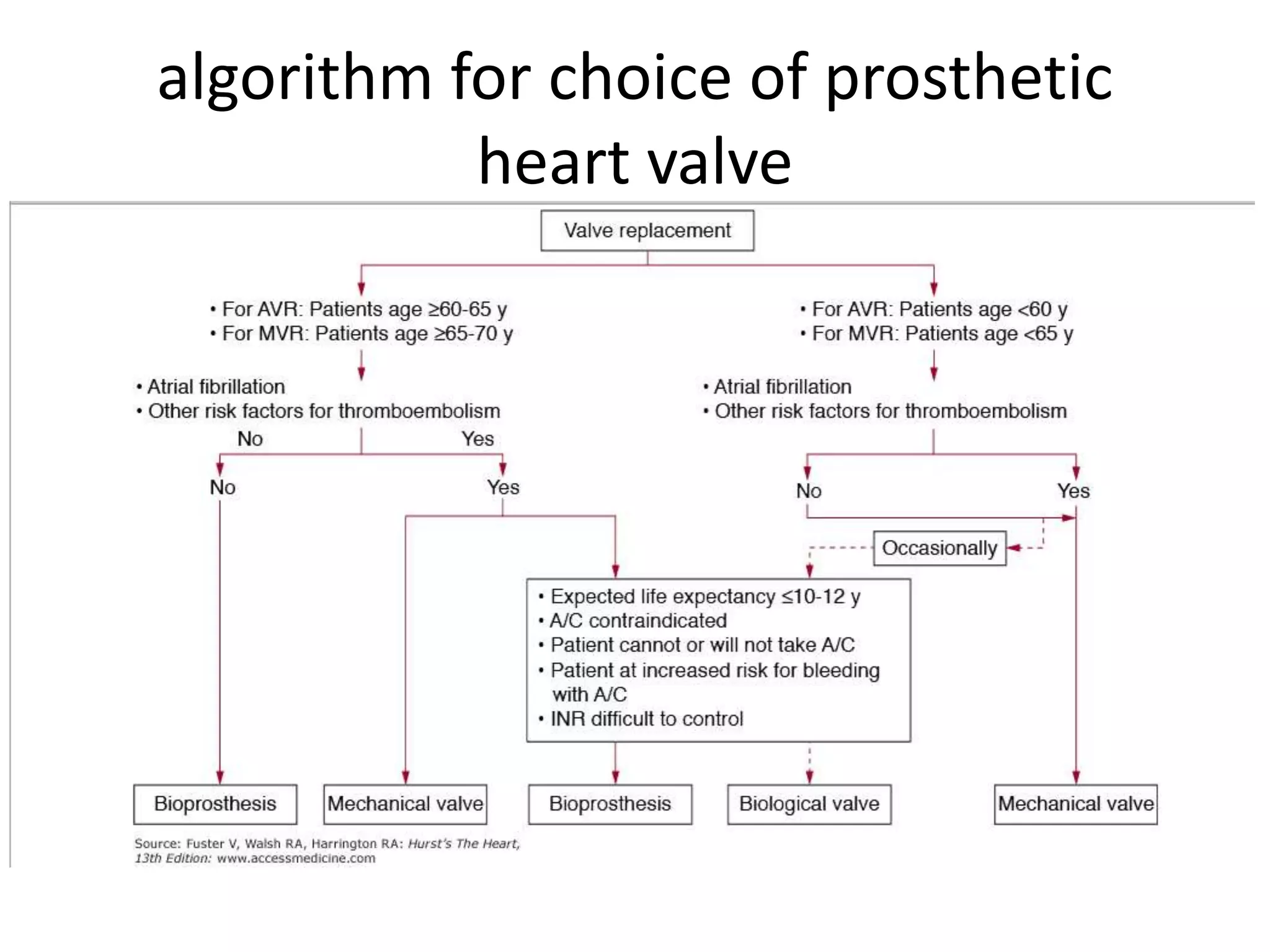
This document discusses types of prosthetic heart valves, including bioprosthetic (tissue) and mechanical valves. It describes the main types of mechanical valves such as caged ball, tilting disc, and bileaflet valves. It provides details on specific valve models and their characteristics. The document also discusses selection criteria for different valve types, complications, diagnostic evaluation using imaging modalities, and management of valve-related issues such as thrombosis.