Downloaded 113 times
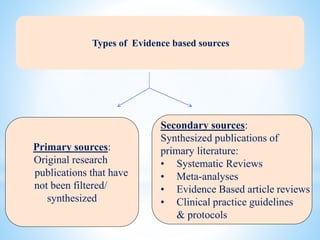
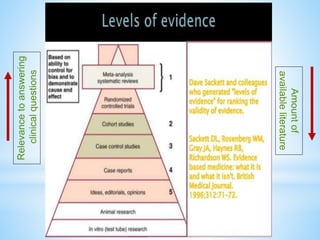
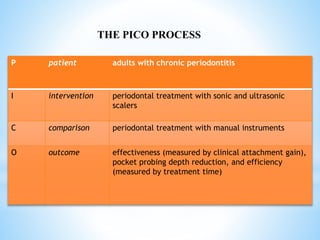
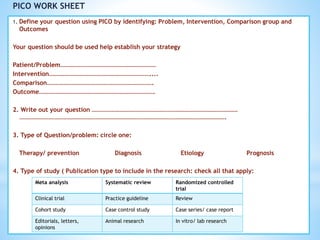
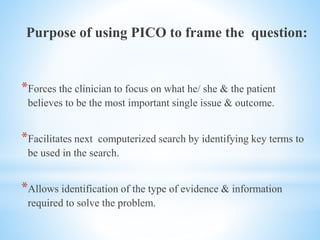
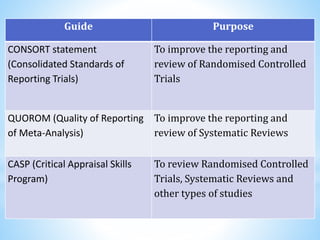



The document provides a comprehensive overview of evidence-based decision making in dentistry, emphasizing the integration of clinical expertise and patient values with the best available research. It discusses the principles, processes, types of evidence, and the need for such an approach to improve healthcare quality while addressing barriers and future implications. Key components include critical appraisal of evidence, the importance of specific questioning techniques like PICO, and the essentials of effective clinical decision-making.





















































































