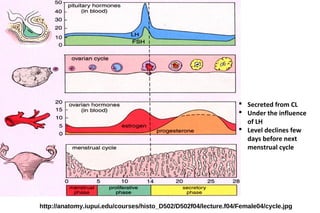
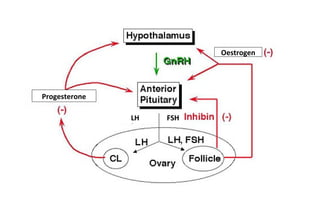
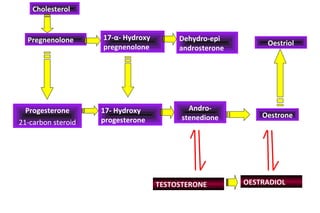
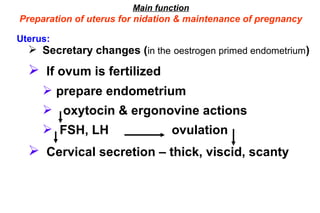
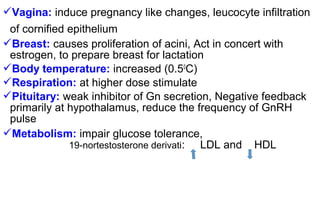
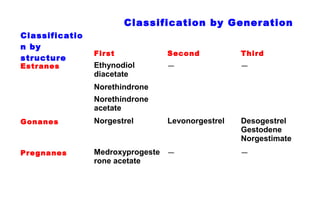
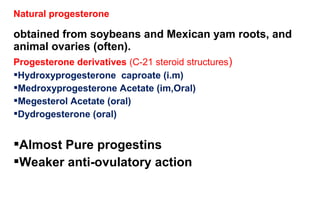
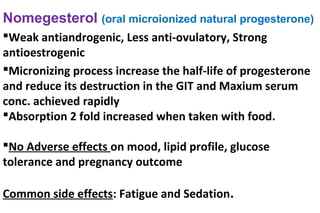
Progestogens are steroid hormones that are synthesized and secreted by the corpus luteum under the influence of LH. Their main function is the preparation of the uterus for implantation and maintenance of pregnancy. They are classified based on their structure and include natural progesterone as well as synthetic derivatives. Common therapeutic uses include oral contraceptives, hormone replacement therapy, dysfunctional uterine bleeding, and endometriosis. Adverse effects may include breast tenderness, headaches, and mood changes. Newer antiprogestins like mifepristone and ulipristal are used for emergency contraception and medical abortion.






















































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)










