Download to read offline


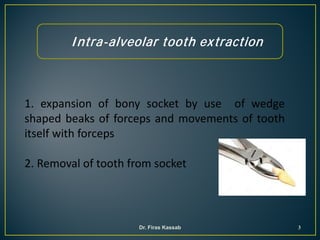
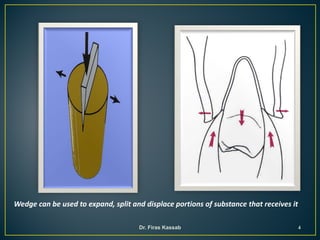
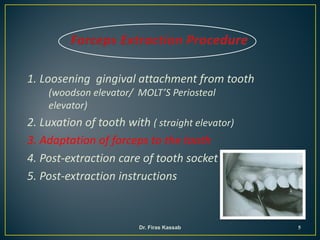

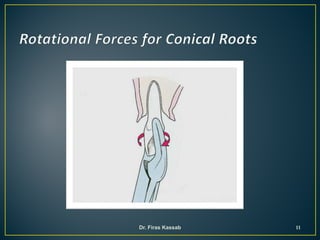
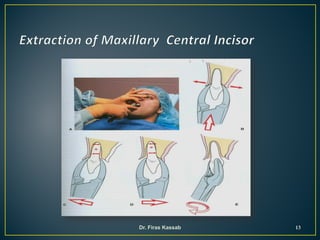
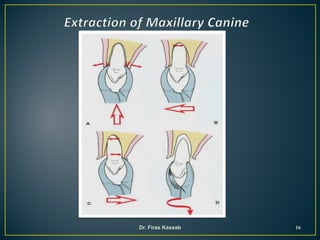
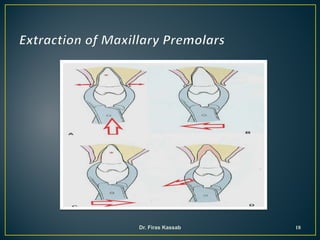
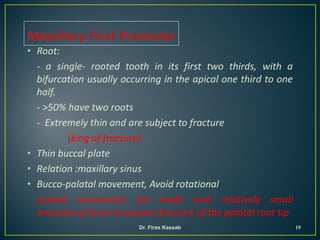

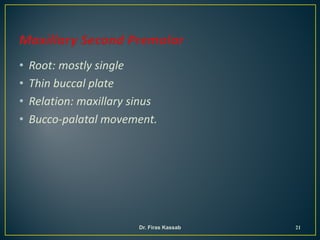
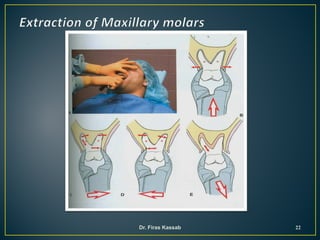
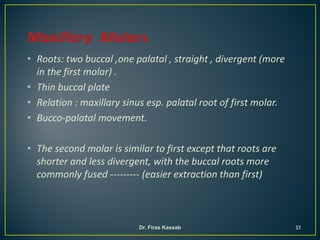

This document discusses the basic techniques for extracting different types of teeth using forceps. It describes how to properly apply forceps to each tooth, focusing the beaks on the difficult surface and as apically as possible. The appropriate movements are outlined for different tooth types, generally starting with firm grip and apical force followed by buccal and lingual movements to expand the socket. Specific techniques are provided for extracting each type of maxillary tooth, noting root morphology, bone thickness, nearby anatomical structures, and recommended extraction movements.












![H.d. ii 09 [1]](https://cdn.slidesharecdn.com/ss_thumbnails/ryg2p6ct2orudqagmmbm-signature-a5fad7992c1f4aa6df744a108dbfc10e79434281f3c12413d51643bf18458881-poli-171206182504-thumbnail.jpg?width=640&height=640&fit=bounds)






























































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)

![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)







