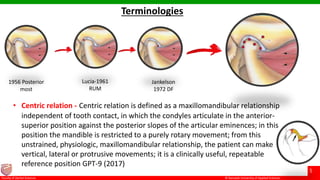
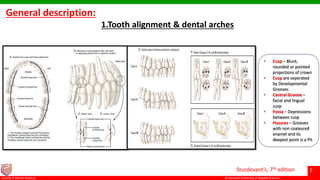
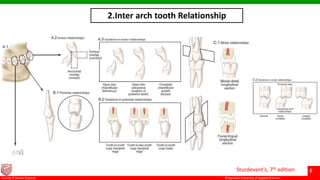
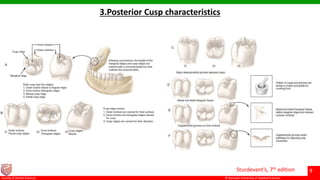
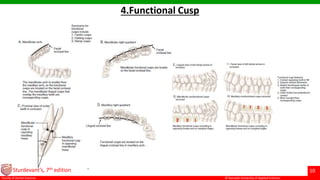

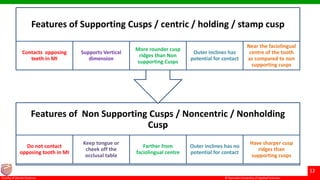
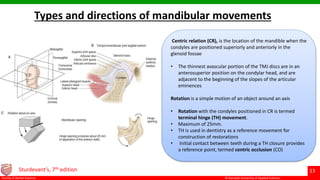
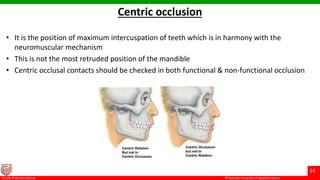
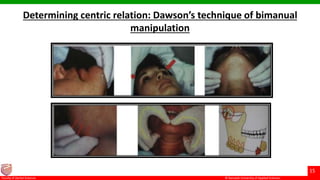

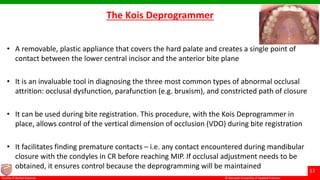
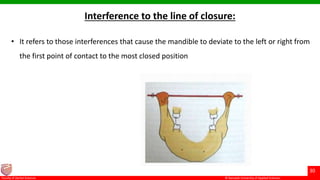
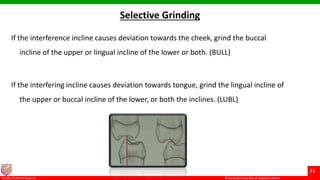







This document discusses occlusion and its relevance to conservative dentistry. It begins with definitions of key terms like centric relation and centric occlusion. It describes tooth anatomy features like cusps, fossae and fissures. It discusses types of tooth contacts during mandibular movements and the role of contacts, contours and marginal ridges in occlusion. It outlines techniques for determining centric relation and recording bite registrations. The document emphasizes that restorations must be made with an understanding of occlusion to avoid problems like tooth pain, muscle tenderness and arthritis.







![Recent advances in direct tooth coloured restoration [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/recentadvancesindirecttoothcolouredrestorationautosaved-210612091304-thumbnail.jpg?width=640&height=640&fit=bounds)