Downloaded 642 times
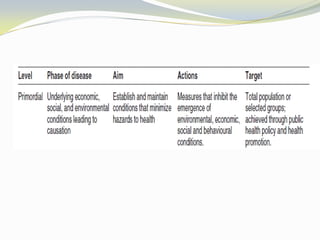
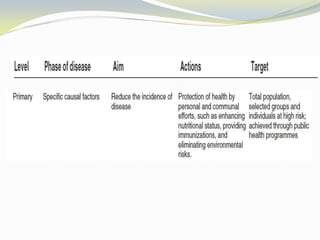
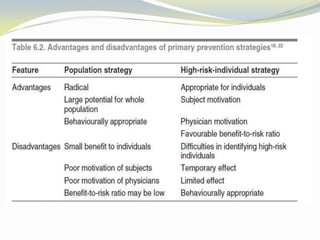

The document discusses the principles and importance of epidemiology, highlighting the role of social determinants in health and disease prevention. It emphasizes that addressing these determinants and employing various levels of prevention can significantly reduce health risks, particularly through primordial and primary prevention strategies. Additionally, it outlines the involvement of diverse professionals in public health and disease prevention efforts.









































![Levels of prevention ppt [pptx -public- health -dentistry]](https://cdn.slidesharecdn.com/ss_thumbnails/dhanashrippt-251029142532-c5df19b7-thumbnail.jpg?width=640&height=640&fit=bounds)




































