Downloaded 11 times



















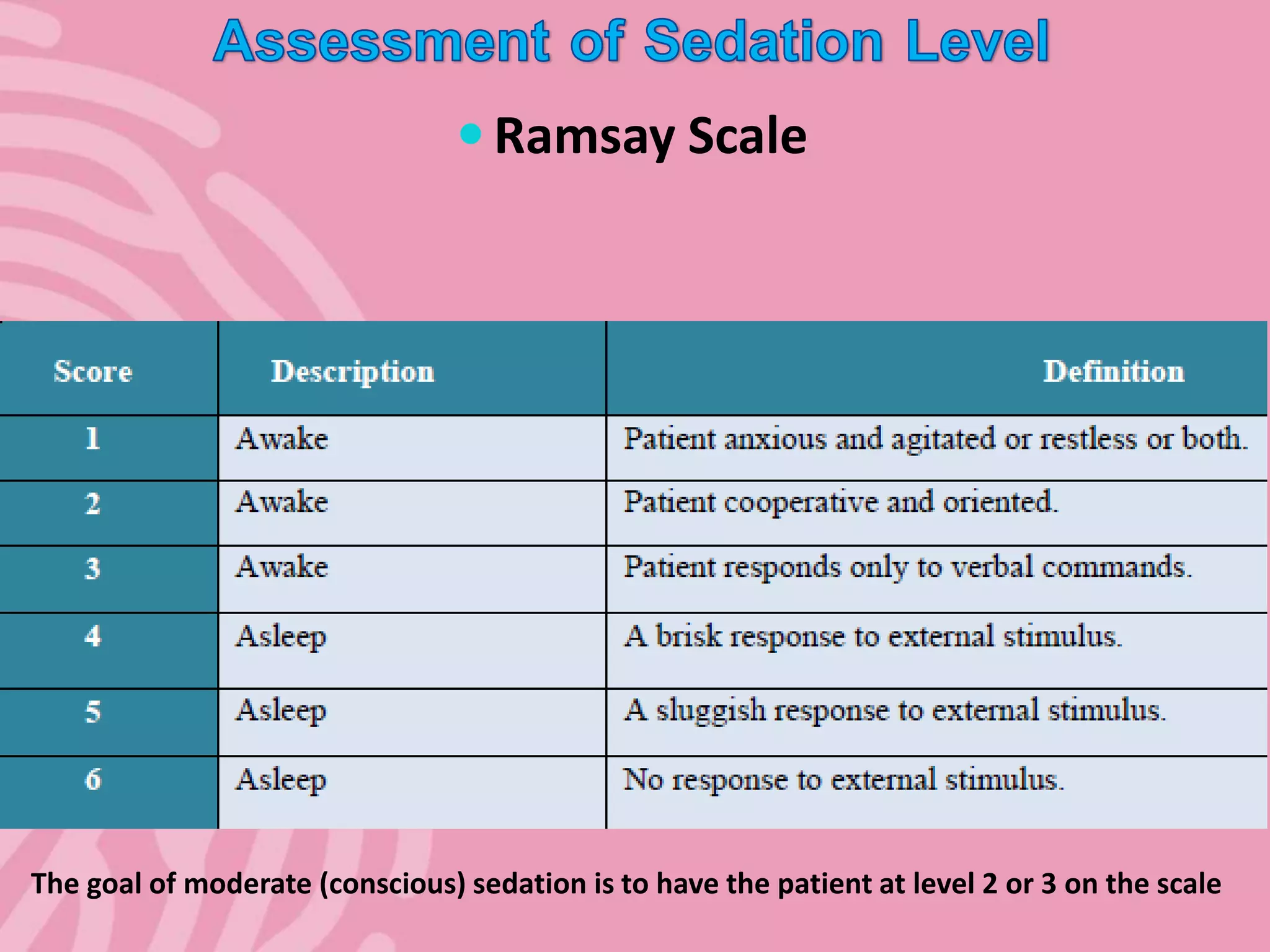





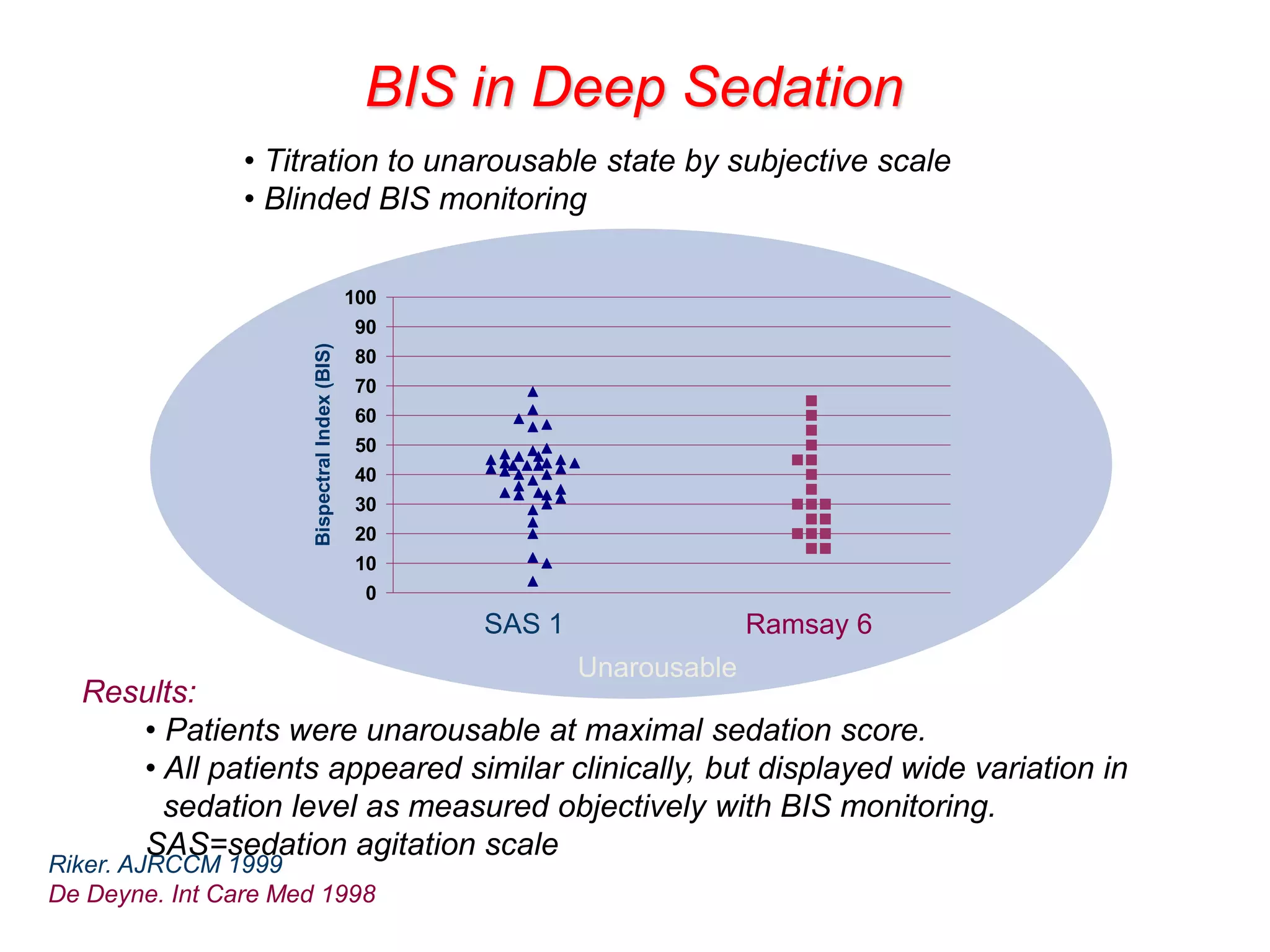





1) The document discusses levels of sedation as defined by the American Society of Anesthesiologists, ranging from minimal sedation to general anesthesia. 2) It emphasizes the importance of understanding sedation levels to provide safe and effective sedation, noting risks like loss of protective reflexes at deeper levels. 3) Continuous monitoring using methods like vital sign checks, sedation scales, and the bispectral index is recommended to properly titrate sedation and avoid under or over-sedation.


































































































