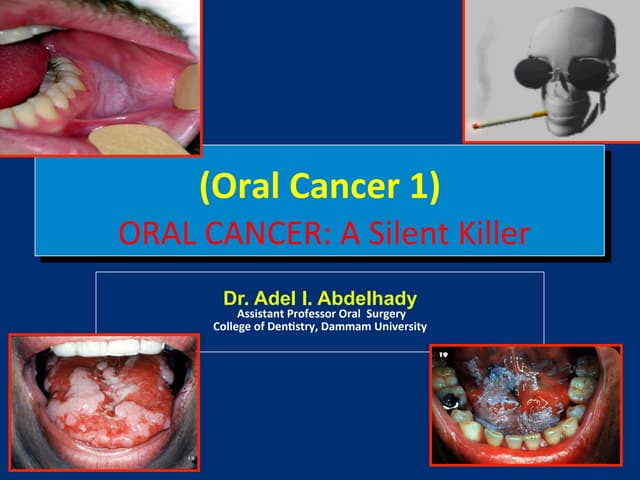
Oral cancer is one of the most common cancers worldwide and constitutes the third most common cancer in developing countries. It affects lips and other intraoral sites. The main risk factors are tobacco, alcohol, poor diet/nutrition, viral infections, and chronic irritation. Precancerous lesions like leukoplakia and erythroplakia can develop due to these risk factors and have a higher risk of becoming cancerous. Prevention focuses on reducing risk factors through education, screening, and early detection/treatment of precancerous lesions. Diagnosis and management depends on the stage, with surgery and radiation used for early stages and palliative care for late stages.