Downloaded 35 times

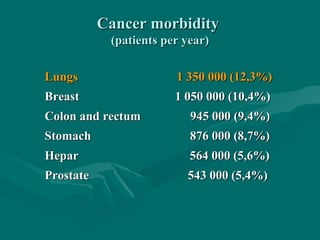


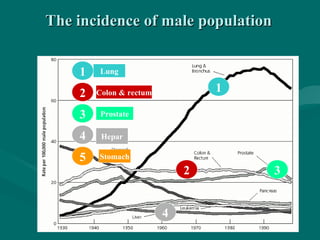
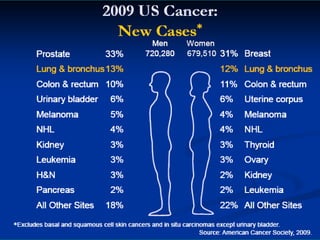
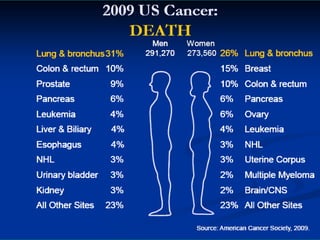

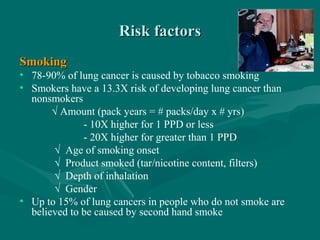


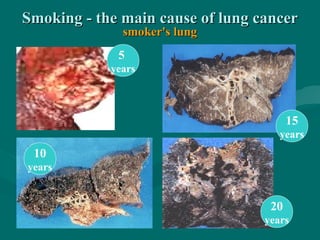
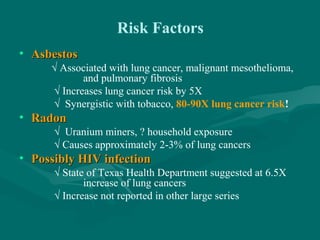

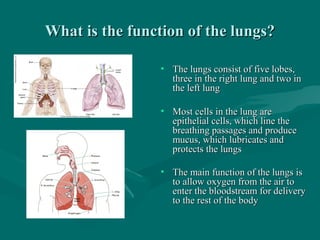
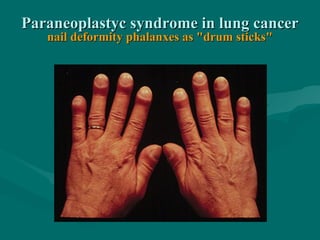
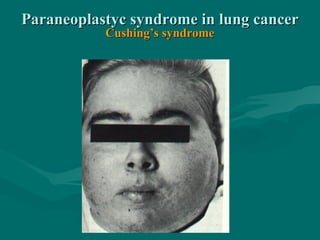

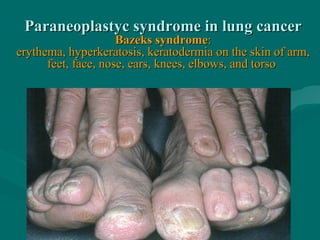
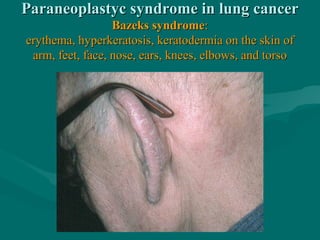


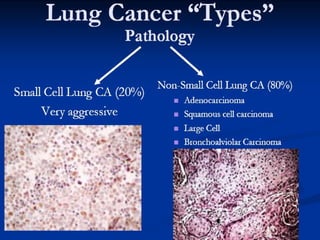
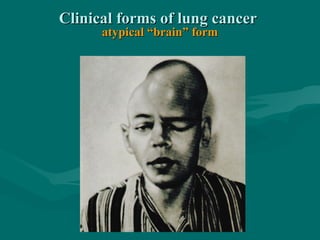
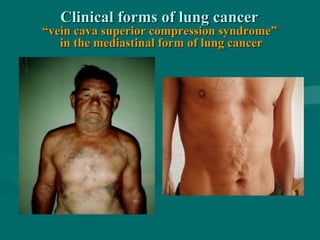
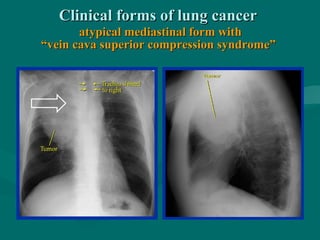
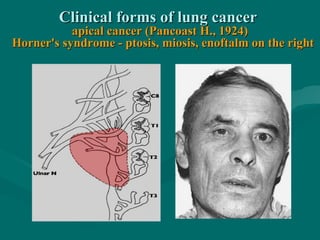







The document discusses lung cancer, which is the leading cause of cancer death worldwide. It estimates that there are 1 million new lung cancer cases each year. Smoking is the primary risk factor, causing 78-90% of lung cancer cases. The document provides statistics on lung cancer incidence and mortality rates around the world. It also discusses risk factors, types of lung cancer, symptoms, functions of the lungs, and paraneoplastic syndromes that can occur in lung cancer patients.























































































