
Downloaded 768 times






























































This document summarizes key information about the management of lung carcinoma: 1. Lung cancer is the leading cause of cancer death worldwide. Smoking is the primary risk factor. Other risk factors include asbestos, radon gas, and genetic mutations. 2. Lung cancers commonly spread to local lymph nodes and distant sites like the brain, bones, liver and adrenal glands. Squamous cell carcinoma and small cell lung cancer often present with central masses while adenocarcinoma presents more peripherally. 3. Staging workup includes chest X-ray, sputum cytology, bronchoscopic biopsy, CT scans, and PET scans to determine the extent of disease for treatment planning.
































































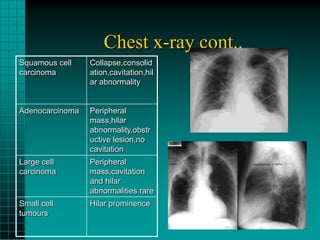
![imaging_in_lung_cancer[1] - Read-Only.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/imaginginlungcancer1-read-only-251017162350-e8ae4014-thumbnail.jpg?width=640&height=640&fit=bounds)



























