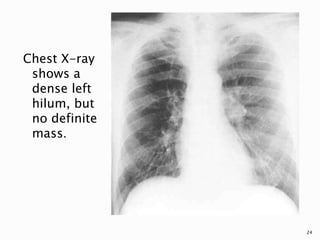
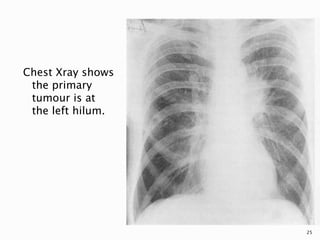
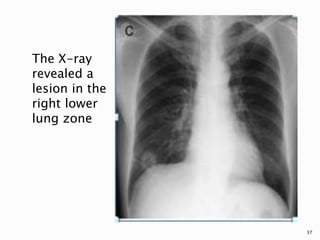
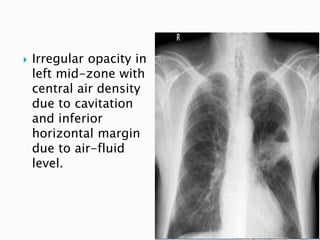
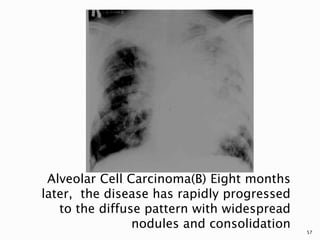
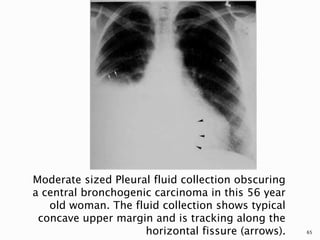
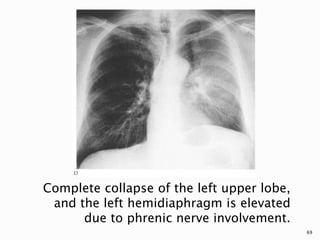
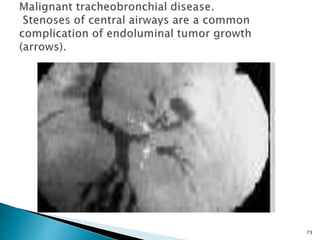
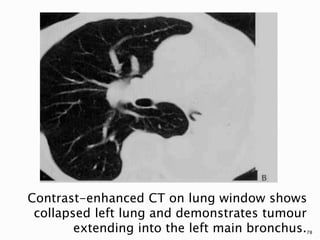
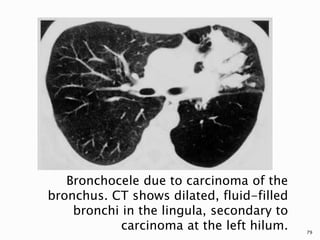
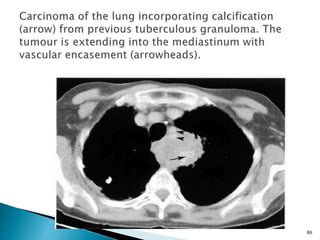
Bronchogenic carcinoma arises from the lung epithelium. It is most common in males aged 40-70 who smoke cigarettes. On chest x-ray, central tumors appear as masses in the hilum while peripheral tumors appear as solitary pulmonary nodules, usually in the upper lobes. Features suggesting malignancy include spiculated margins, lobulation, cavitation with thick walls, and growth over time. Radiography remains important for initial detection and assessment of complications.

![ One of the more recent advances in
oncologic imaging that has generated a
renewed interest in diagnosis, staging, and
response to therapy is positron emission
tomography (PET).
PET imaging with [2-18F]fluoro-2-deoxy-
D-glucose (F-18 FDG) allows for the
evaluation of the relative level of metabolic
activity of a lesion compared with other
tissues.
123](https://image.slidesharecdn.com/bronchogeniccarcinoma-150504100413-conversion-gate02/85/Bronchogenic-carcinoma-123-320.jpg)