Download as PDF, PPTX

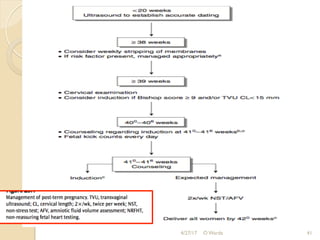

This document discusses post-term pregnancy, defined as a pregnancy extending beyond 42 weeks of gestation. It covers the epidemiology, etiology, risk factors, morbidity and mortality, diagnosis, and management of post-term pregnancies. The key points are: 1. The incidence of post-term pregnancy varies from 0.4-8.1% depending on location and methods of assessing gestational age. The causes are often unknown but may involve genetic or placental factors. 2. Risk factors include prior post-term pregnancy, nulliparity, advanced maternal age, obesity, male fetus, and inaccurate dating. Post-term pregnancies have higher risks of complications like macrosomia, dysmaturity syndrome





































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)

















