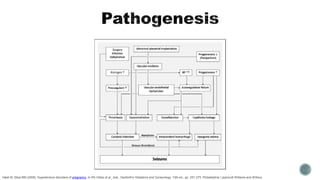
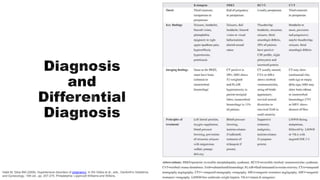
This document discusses preeclampsia and eclampsia. It defines preeclampsia as new-onset hypertension and proteinuria during pregnancy. Eclampsia occurs when seizures develop in the setting of preeclampsia. Late postpartum eclampsia, which can occur up to 6 weeks after delivery, is rare. Magnesium sulfate is the primary treatment for eclampsia, as it helps prevent seizures by blocking calcium channels in the brain. Eclampsia can cause major morbidity and mortality for both mother and baby.