DEFINITION :
Post termpregnancy is defined as ≥42 weeks of
gestation (≥294 days from the first day of the last
menstrual period and ≥14 days from the estimated day
of delivery).
3.
Women at highestrisk of
post term pregnancy are
those with a previous
post term pregnancy.
04
RISK FACTORS
06
01
03
Obesity
Maternal (and to a
lesser extent paternal)
personal history of
post term brith.
02 Nulliparty 05 Older maternal age
Male fetus
The diagnosis ofpregnancy 42weeks of
≥
gestation is based on the clinician's most
accurate estimate of the patient's delivery date
(EDD). For most pregnancies, the most accurate
EDD is based on an ultrasound examination
performed before 22weeks of gestation if this
EDD differs from that calculated from menstrual
dating by more than expected.
DIAGNOSIS
6.
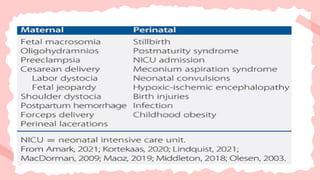
Post term pregnancyis associated with maternal,
fetal, and neonatal complications.
Many of the complications are sequelae of either
excessive fetal growth or placental insufficiency.
MORBIDITY AND MORTALITY
8.
Most post termfetuses are larger than term
fetuses, with a higher incidence of macrosomia
( 4500 g) because of the longer duration of
≥
intrauterine growth.
Macrosomia increases the risks for several adverse
sequelae, including abnormal labor progression,
cesarean delivery, assisted vaginal delivery,
shoulder dystocia, maternal/fetal/newborn birth
injury, postpartum hemorrhage, and neonatal
metabolic problems.
Macrosomia
9.
In contrast, upto 20 percent of post term fetuses have "fetal
dysmaturity (postmaturity) syndrome, a term used to describe
fetuses with characteristics of chronic intrauterine malnutrition.
These fetuses are at increased risk of umbilical cord
compression due to oligohydramnios, and abnormal
antepartum or intrapartum fetal heart rate patterns due to
placental insufficiency or cord compression. Meconium passage
is common and may be related to physiological maturation of
the gut or fetal hypoxia.
Dysmaturity
10.
Affected neonates havea long thin body, long nails, and are
small for gestational age. Their skin is dry (vernix caseosa is
decreased or absent), meconium-stained, parchment-like,
and peeling; it appears loose, especially over the thighs and
buttocks, and has prominent creases; lanugo hair is sparse
or absent, while scalp hair is increased.
Con..
11.
These neonates areat risk for morbidities
associated with growth restriction, including
hypoglycemia, polycythemia, perinatal asphyxia,
meconium aspiration, and persistent pulmonary
hypertension. They are also at risk for
neurodevelopmental complications (eg,
seizures, cerebral palsy
Con..
12.
The perinatal mortalityrate at 42 weeks of gestation is twice
≥
the rate at term, increasing fourfold at 43 weeks, and five- to
sevenfold at 44 weeks .
Perinatal mortality increases as pregnancy extends beyond full
term, particularly after 41 weeks, due to increases in both no
anomalous stillbirths and early neonatal deaths. Intrauterine
infection, placental insufficiency due to placental aging, and
cord compression leading to fetal hypoxia, asphyxia, and
meconium aspiration are thought to contribute to the excess
perinatal deaths
Perinatal mortality
13.
It is unclearwhether, or to what degree, perinatal mortality is
increased in post term pregnancies without fetal
malformations, signs of placental insufficiency (growth
restriction, oligohydramnios), or maternal disorders
associated with adverse pregnancy outcome (eg, diabetes,
hypertension) .
Con..
14.
The following discussionrefers to the singleton, cephalic
fetus of an otherwise uncomplicated pregnancy that
reaches 41 weeks of gestation. Multiple gestations, non-
cephalic presentations, and pregnancies with medical or
obstetric complications are generally delivered before 41
weeks .
MANAGEMENT
15.
Pregnancies that reach41 weeks of gestation can be induced or
managed expectantly with ongoing fetal assessment and
intervention if spontaneous labor does not occur by a
predefined gestational age or fetal assessment is not
reassuring.
In the low-risk post term gravida, both of these approaches are
associated with low rates of adverse outcome. Patients should
be counseled about what these approaches involve (labor
induction with/without cervical ripening agents, type and
frequency of antepartum fetal and maternal monitoring) and
the maternal and fetal benefits and risks of both approaches.
Con..
16.
Expectant management isthe alternative to induction.
Expectantly managed pregnancies typically undergo twice-weekly
fetal assessment beginning at 41 weeks or shortly thereafter, with
intervention if spontaneous labor does not occur by a predefined
gestational age or fetal assessment testing is abnormal.
Either a nonstress test plus assessment of amniotic fluid volume
or the biophysical profile can be used for antenatal monitoring;
there is no convincing evidence that one method is superior to the
other.
Expectant management with
fetal monitoring
17.
We agree withthe American College of Obstetricians and
Gynecologists recommendation to induce labor by 42+6
weeks of gestation in all pregnancies . Earlier induction is
indicated for development of any of the usual obstetrical
indications, including evidence of oligohydramnios Adverse
pregnancy outcomes (abnormal fetal heart rate tracing,
neonatal intensive care unit admission, low Apgar) are more
likely when oligohydramnios is present.
Timing of delivery in expectantly
managed pregnancies
18.
Because so fewpregnancies reach 43 weeks, there is no
strong evidence on which to base a recommendation for
the maximum gestational age at which an otherwise
uncomplicated pregnancy should be delivered in the
absence of standard maternal or fetal indications or
spontaneous labor.
Con..
19.
As discussed above, after one post term pregnancy, the risk of
a second post term birth is increased two- to fourfold; the risk
of recurrence is higher after two prior post term pregnancies .
As an example, in the Netherlands Perinatal Registry database
of over 230,000 women with singleton pregnancies who
delivered their first pregnancy at 37+0 to 42+6 weeks of
gestation and had a subsequent singleton pregnancy, post
term births occurred in 7.7 percent of first pregnancies, 15
percent of second pregnancies in women who had a previous
postterm birth, and in 4 percent of second pregnancies in
women who had a previous term birth .
RECURRENCE RISK