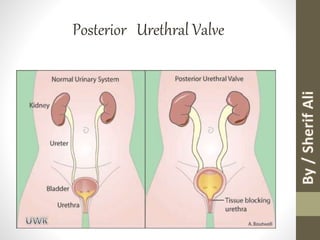
4. - A (PUV) is an abnormal congenital obstructing
membrane that is located within the posterior male
urethra; this valve is the most common cause of
bladder outlet obstruction in male children. [1, 2, 3]
5. - The valve is believed to result from abnormal
embryologic development of the fetal posterior
urethra.
- These valves essentially obstruct normal bladder
emptying. This mechanical obstruction increases
voiding pressures and may alter normal
development of the fetal bladder and kidneys.
6.
7. - Children with higher degrees of obstruction
present earlier with the most severe
symptoms.
- A spectrum of signs and symptoms, ranging
from mild obstructive symptoms of voiding
dysfunction to severe obstruction with resultant
renal failure and pulmonary hypoplasia , may be
noted. (3)
9. Incidence :
- 1 per 5000 to 8000
- More than 50 % are diagnosed in the 1st year
with more severe obstruction .
10. - Renal insufficiency is caused by PUVs in
approximately 10-15 % of children
undergoing renal transplant .
- approximately 1/3 of patients born with
PUVs progress to end stage renal disease
(ESRD)
13. - The classic categorization of
posterior urethral valves into
types I, II, and III was
developed by H. H. Young in
1919[4] and has undergone
modification over time based
on clinical observation and a
better understanding of the
embryologic events that lead to
normal urethral development.
14. Type I PUV
- Type I valve accounts for 95 % of all valves
- Secondary to abnormal insertion and absorption of most distal
aspects of the Wolffian ducts during bladder development .
15. - Bicuspid valve that radiates distally from the
posterior edge of the verumontanum to the anterior
proximal membranous urethra
16. Type II PUV
- Very infrequent
- Non obstructive urethral
folds
- It's thought to be a sequela of
voiding dysfunction ,
- therefore these valves can
be differentiated from Type I
& Type III valves by their
location proximal to the
verumontanum (extends
proximaly from the
verumontanum to the
17. Type III PUV
- Membrane in the posterior
urethra believed to originate
from incomplete canalization
between the anterior &
posterior urethra.
- This valve is a
circumferential membrane or
diaphragm that is located at
the membranous urethra .
- Type III valves account for
almost 5 % of all valves
20. Voiding cystourethrogram
(VCUG)
is the best imaging technique for the
diagnosis of PUV and can show :
- visualizations of the valve
leaflets
- Thickened & trabeculated
bladder
- Dilated or elongated posterior
urethra
- Hypertrophied bladder neck
- Diverticula
- vesicoureteral reflux and
reflux into the ejaculatory
ducts secondary to elevated
bladder and urethral pressure
24. Antenatal & Postnatal Ultrasound
- Marked distention and hypertrophy of the bladder
- Hydronephrosis and hydroureter may or may not be present
- In severe cases oligohydramnios and renal dysplasia (2)
- Keyhole sign may be seen on ultrasound due to the distention of
both the bladder and the urethra immediately proximal to the valve(5) .
** Unfortunately, such findings are generally not seen before 26 weeks
of gestation. (5)
25.
26.
27. Delayed presentation
- UTI
- Diurnal enuresis in boys older than 5 years
- Secondary diurnal enuresis
- Voiding pain or dysfunction
- Decreased force of stream may indicate the
presence of PUVs
- Discovered during evaluations of abdominal mass
or renal failure.
28. Differential Diagnosis
- In this age group and with clear dilatation of the
posterior urethra there is usually little differential other
than urethral atresia, which is far less common (2).
- When only the bladder is clearly abnormal - thick walled
and trabeculated, other conditions to be considered
include (5):
* Neurogenic bladder
* Prune-belly syndrome
36. - PUV has 3 types I , II &III
- Type I is the most common , Type III has the worst
prognosis.
- A spectrum of signs and symptoms, ranging from mild
obstructive symptoms of voiding dysfunction to severe
obstruction with resultant renal failure and pulmonary
hypoplasia.
- Long term sequelae are significant especially renal
disease.
- VCUG is the best modality of diagnosis.
- Majority are managed by valve ablation