Etiology
• shoulder jointdislocates more frequently than any other joint in the
body.
• A dislocation can become worse by strained or torn fibrous tissue
which connects the bones.
• Contact sports injury are a common cause a dislocated shoulder as
are motor trauma and falls.
5.
Epidemiology
• Shoulder jointdislocations are the most common dislocations of all major
joint dislocations.
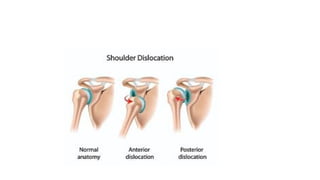
• Shoulder dislocations can be Anterior and Posterior dislocations.
Risk factors for re-dislocation:
• Prior dislocation with poor tissue healing or soft issue laxity
• Younger patients have a much higher frequency of re-dislocation as they are
more active
• Patients with torn rotator cuffs or fracture of the glenoid have a higher
incidence of re-dislocation.
6.
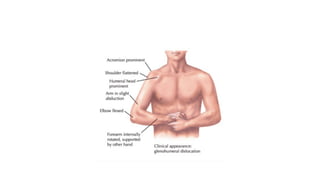
Clinical presentation?
Anterior Dislocation
•humeral head comes to lie anterior, medial and slightly inferior to its normal location
• Arm held in an abducted and ER position
• Loss of normal contour of the deltoid and acromion prominent posteriorly and laterally
• Humeral head palpable anteriorly
• All movements limited and painful
• Palpable fullness below the coracoid process and towards the axilla
• Possible damage to rotator cuff musculature and bone.
• Vascular injuries may result from traction of the axillary blood vessels, resulting in a
reduced pulse pressure or a transient coolness in the hands.
• Peripheral nerve injuries are common due to traction if the brachial plexus.
8.
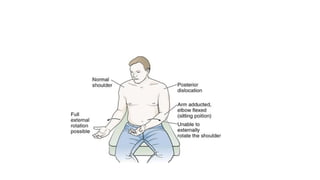
Posterior Dislocation
• Withacute posterior glenohumeral dislocation:
• Arm is abducted and IR
• May or may not lose deltoid contour
• May notice posterior prominence head of humerus
• Tear of subscapularis muscle (weak or cannot internally rotate)
• Neurovascular compromise is rare, but posterior shoulder instability may result from associated
glenolabral and capsular injuries.
• Posterior dislocations are hard to reduce, attempts at closed reduction need be performed in
consultation with a treating orthopaedic surgeon.
• Shoulder dislocation was ≥3 weeks ago (common in feeble elderly patients) or if their is reverse
Hill-Sachs defect involving >20% of the articular surface, then the closed reduction is
contraindicated
10.
Diagnosis ?
• X-rayare is often enough to make a diagnosis of shoulder dislocation, however CT
and MR are often needed to assess for the presence of subtle fractures of the
glenoid rim or ligamentous/tendinous injuries respectively.
• Clinical
11.
Management
Anterior Dislocation
closed reductionand a period of immobilisation (e.g. 6 weeks), allowing for adequate capsular healing. For successful healing and eventual normal function a structured
course of physical therapy is needed to reduce muscle wasting and maintain mobility.
• Following traumatic ASD, there is great variability in the post-operative immobilisation period and at which stage each type of exercise is introduced.
Phase 1 Immobilisation (up to 6 weeks)
Goal is to maintain anterior-inferior stability
• Typical time periods in a sling range for 3-6 weeks if under the age of 40 and 1-2 weeks if older than the age of 40.[12]
• During the immobilization period, the focus is on AROM of the elbow, wrist and hand and reduction of pain. Isometrics can be incorporated for the rotator cuff and biceps
musculature.
Phase 2 (6-12 weeks)
Goal is to restore adequate motion, specifically in external rotation
• AAROM to achieve a full range of motion when stretching is permitted, passively stretch the posterior joint capsule through the use of joint mobilizations or self-
stretching.
• No strengthening or repetitive exercises should start until the achievement of the full range of motion
Phase 3 (12-24 weeks)
Successful return to sports or physical activities of daily living
• Begin strengthening exercise
• A possible progression could begin by focusing on the rotator cuff musculature and scapular stabilizers, which include trapezius, serratus, levator scapulae, and
rhomboids. Then, progress to the larger musculature such as the deltoids, latissimus dorsi, and pectorals.
• Start focusing on functional exercises include proprioceptive training, tailor to promote patient's activities and participation in society
12.
Posterior Dislocation
• Managementfor posterior dislocation follows the same progression
as anterior protocol, except for the following guidelines:
a. Posterior glide is contraindicated
b. Avoid flexion with adduction and internal rotation
c. Immobilized 3-6 weeks if less than 40 years of age and 2-3 weeks if
greater than 40 years of age
d. Strengthening will focus primarily on posterior musculature such
as: infraspinatus, teres minor and posterior deltoid

![Management
Anterior Dislocation
closed reduction and a period of immobilisation (e.g. 6 weeks), allowing for adequate capsular healing. For successful healing and eventual normal function a structured
course of physical therapy is needed to reduce muscle wasting and maintain mobility.
• Following traumatic ASD, there is great variability in the post-operative immobilisation period and at which stage each type of exercise is introduced.
Phase 1 Immobilisation (up to 6 weeks)
Goal is to maintain anterior-inferior stability
• Typical time periods in a sling range for 3-6 weeks if under the age of 40 and 1-2 weeks if older than the age of 40.[12]
• During the immobilization period, the focus is on AROM of the elbow, wrist and hand and reduction of pain. Isometrics can be incorporated for the rotator cuff and biceps
musculature.
Phase 2 (6-12 weeks)
Goal is to restore adequate motion, specifically in external rotation
• AAROM to achieve a full range of motion when stretching is permitted, passively stretch the posterior joint capsule through the use of joint mobilizations or self-
stretching.
• No strengthening or repetitive exercises should start until the achievement of the full range of motion
Phase 3 (12-24 weeks)
Successful return to sports or physical activities of daily living
• Begin strengthening exercise
• A possible progression could begin by focusing on the rotator cuff musculature and scapular stabilizers, which include trapezius, serratus, levator scapulae, and
rhomboids. Then, progress to the larger musculature such as the deltoids, latissimus dorsi, and pectorals.
• Start focusing on functional exercises include proprioceptive training, tailor to promote patient's activities and participation in society](https://image.slidesharecdn.com/shoulderdislocation-250827002700-08afd994/85/Shoulder-Dislocation-anterior-and-posterior-11-320.jpg)