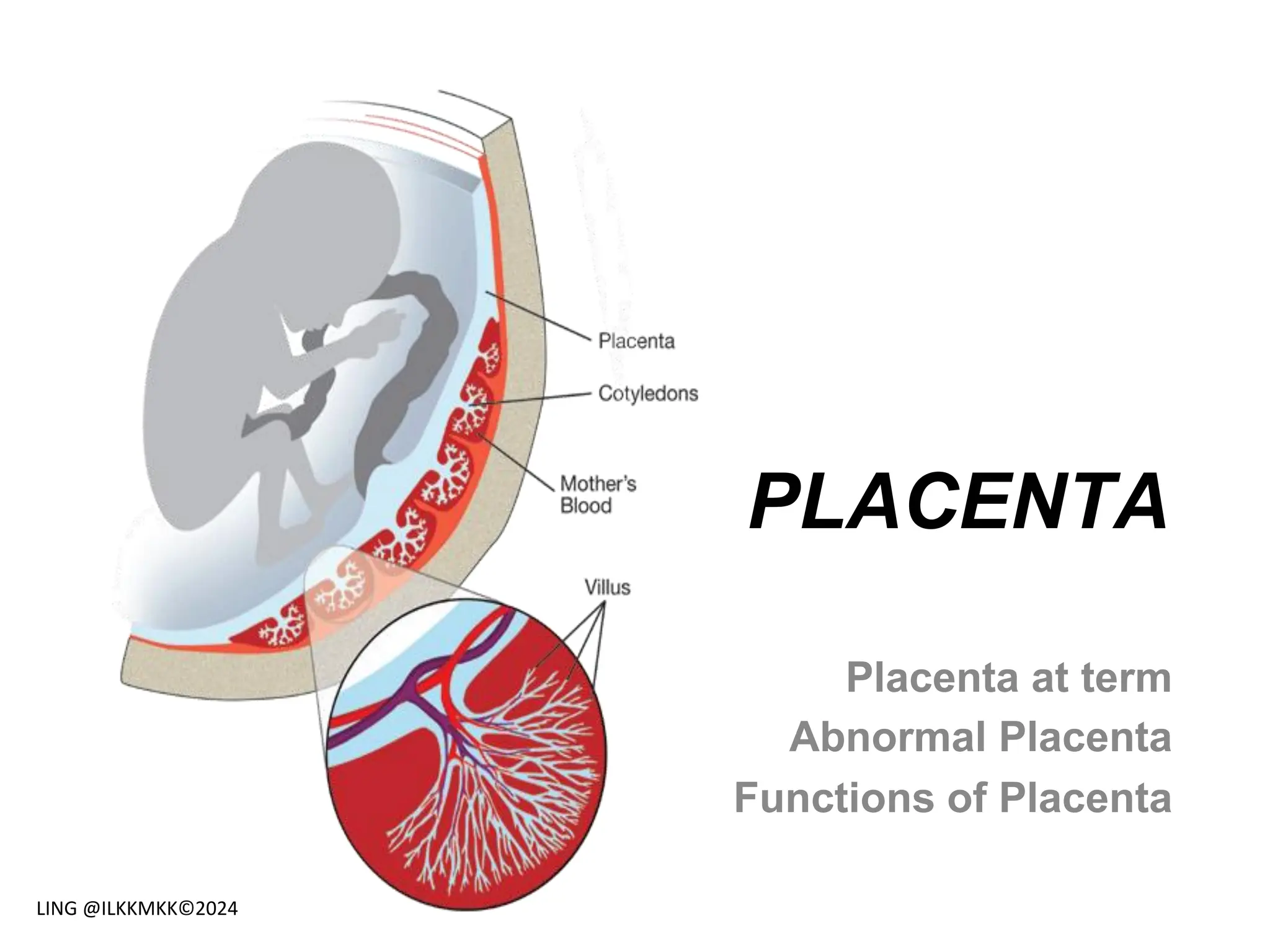
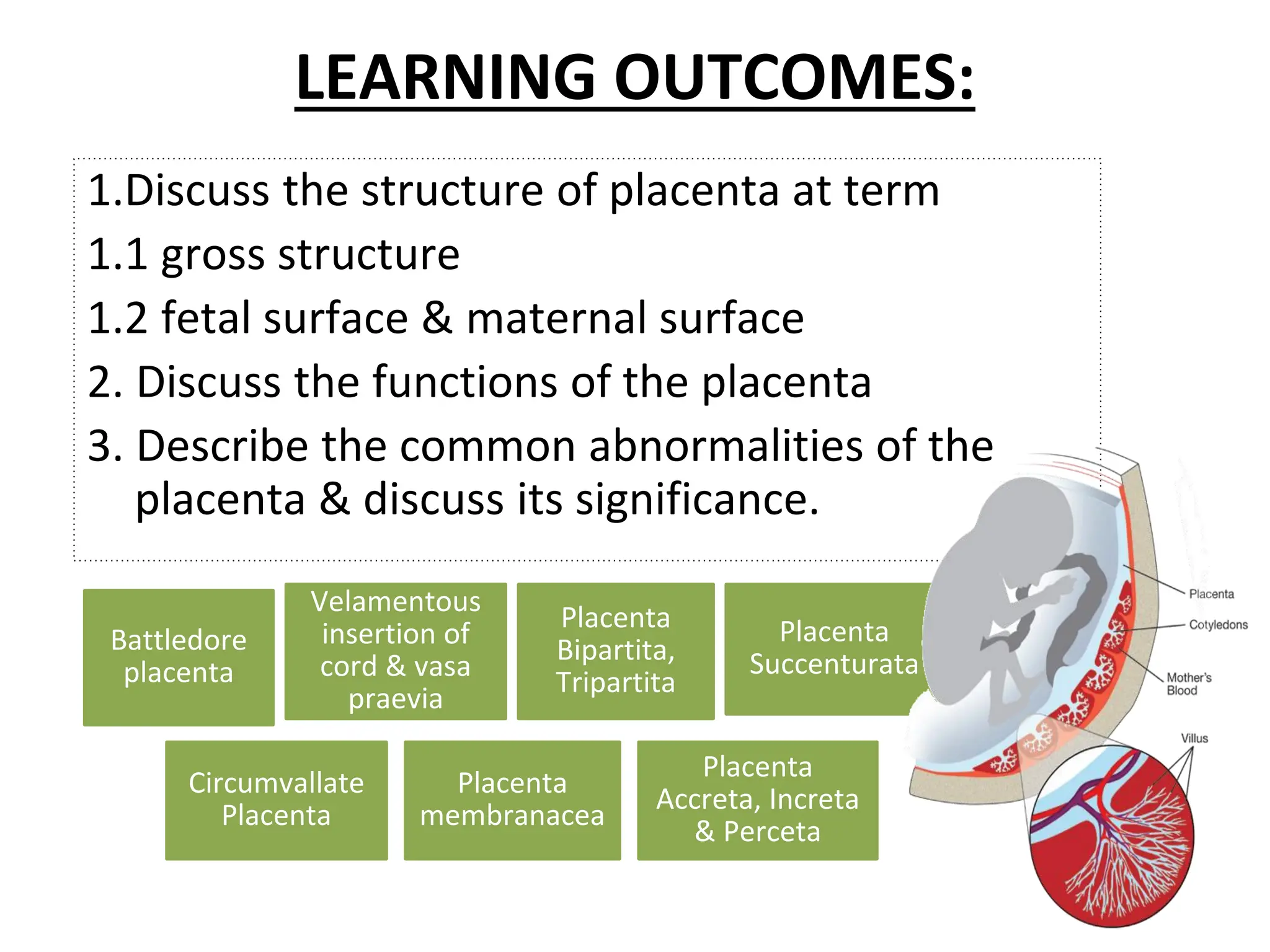
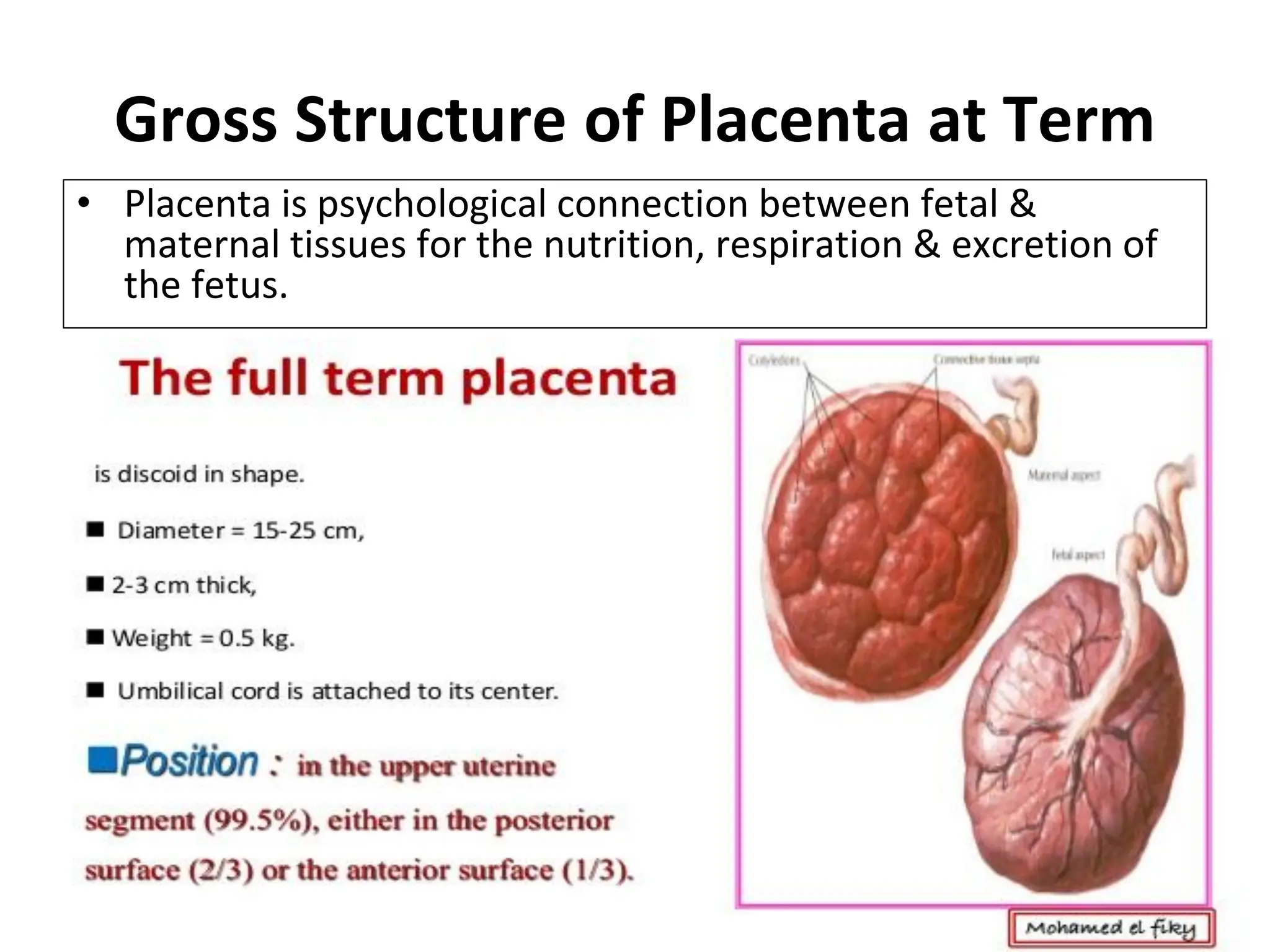
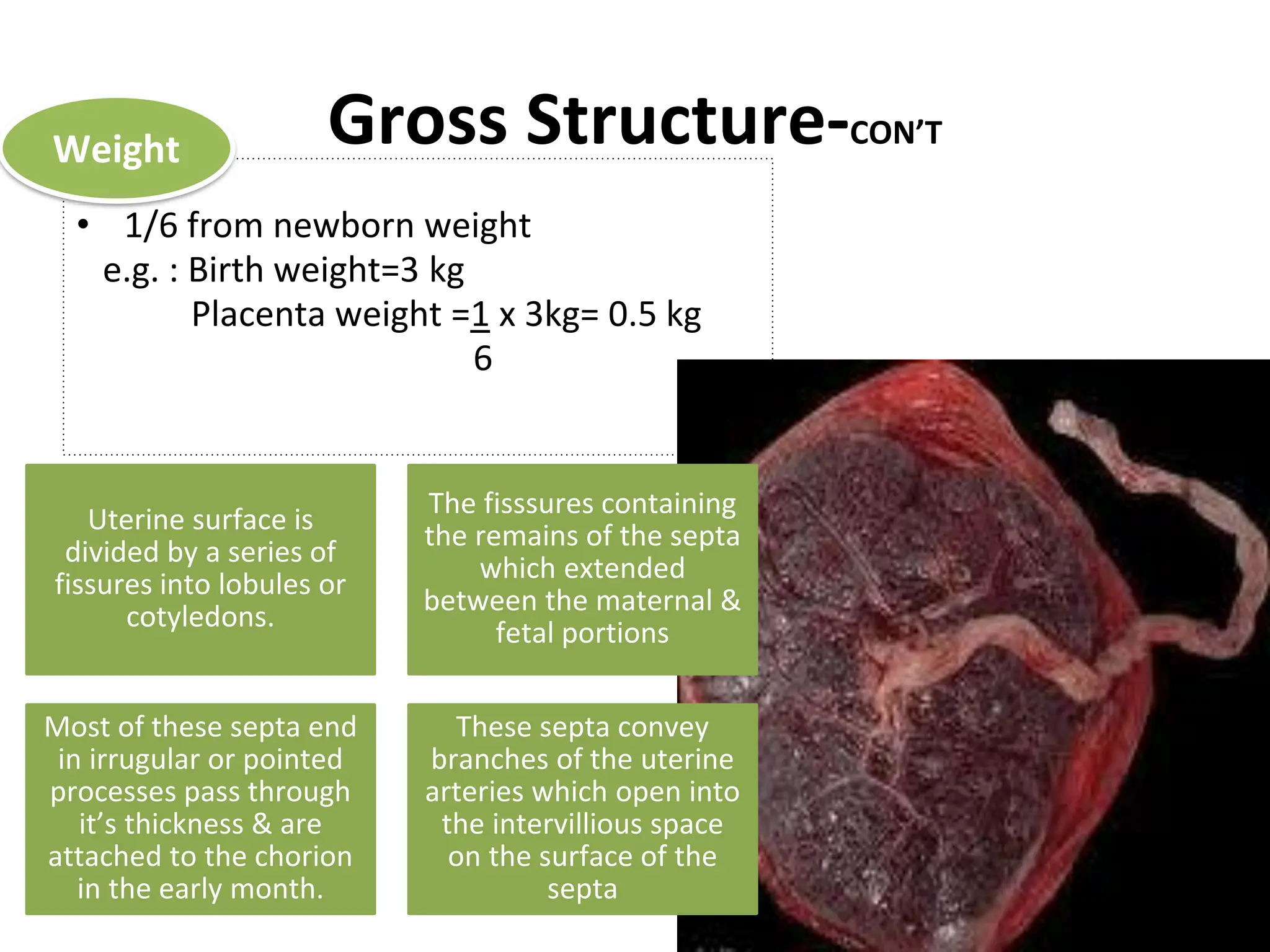
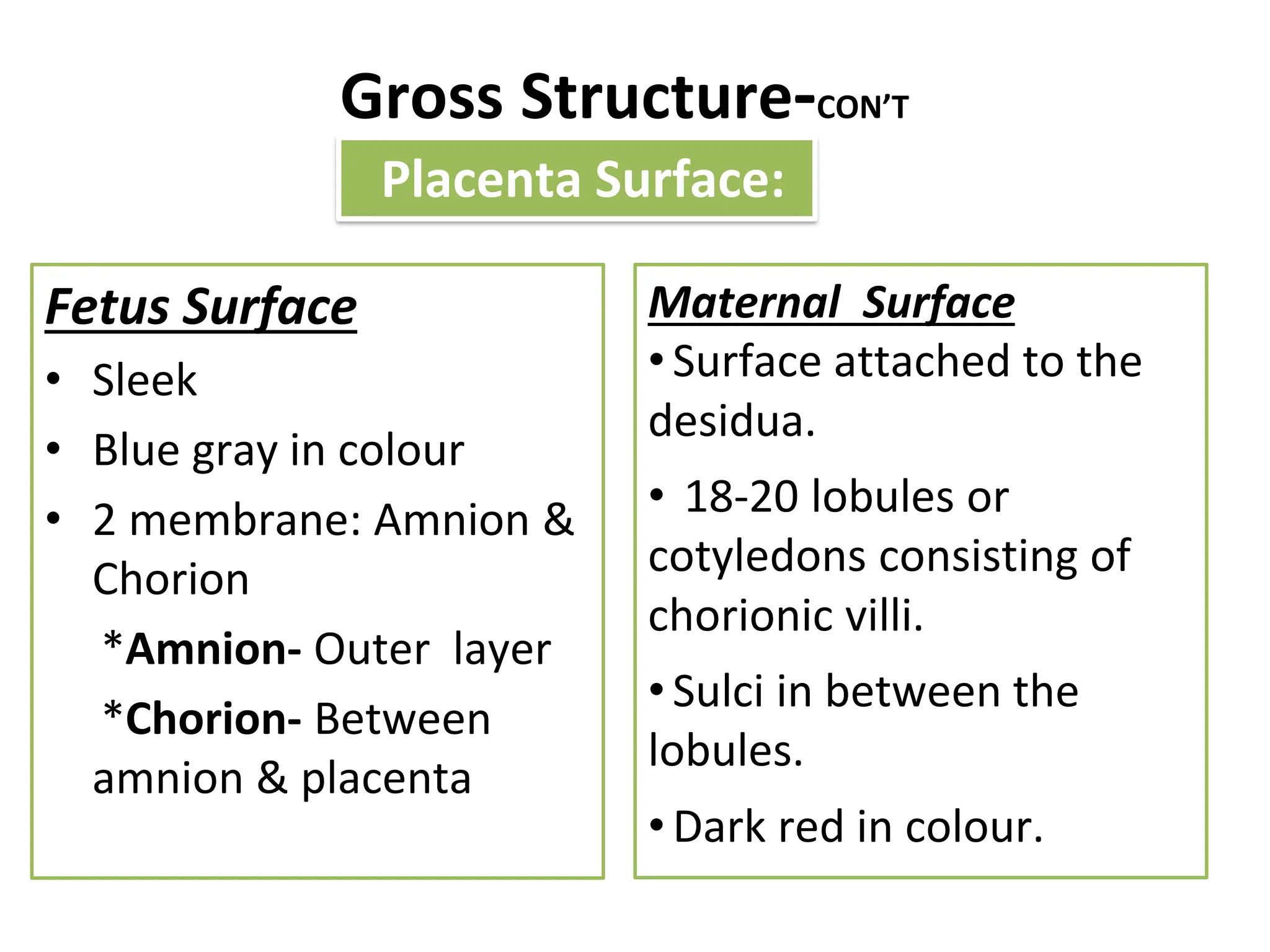
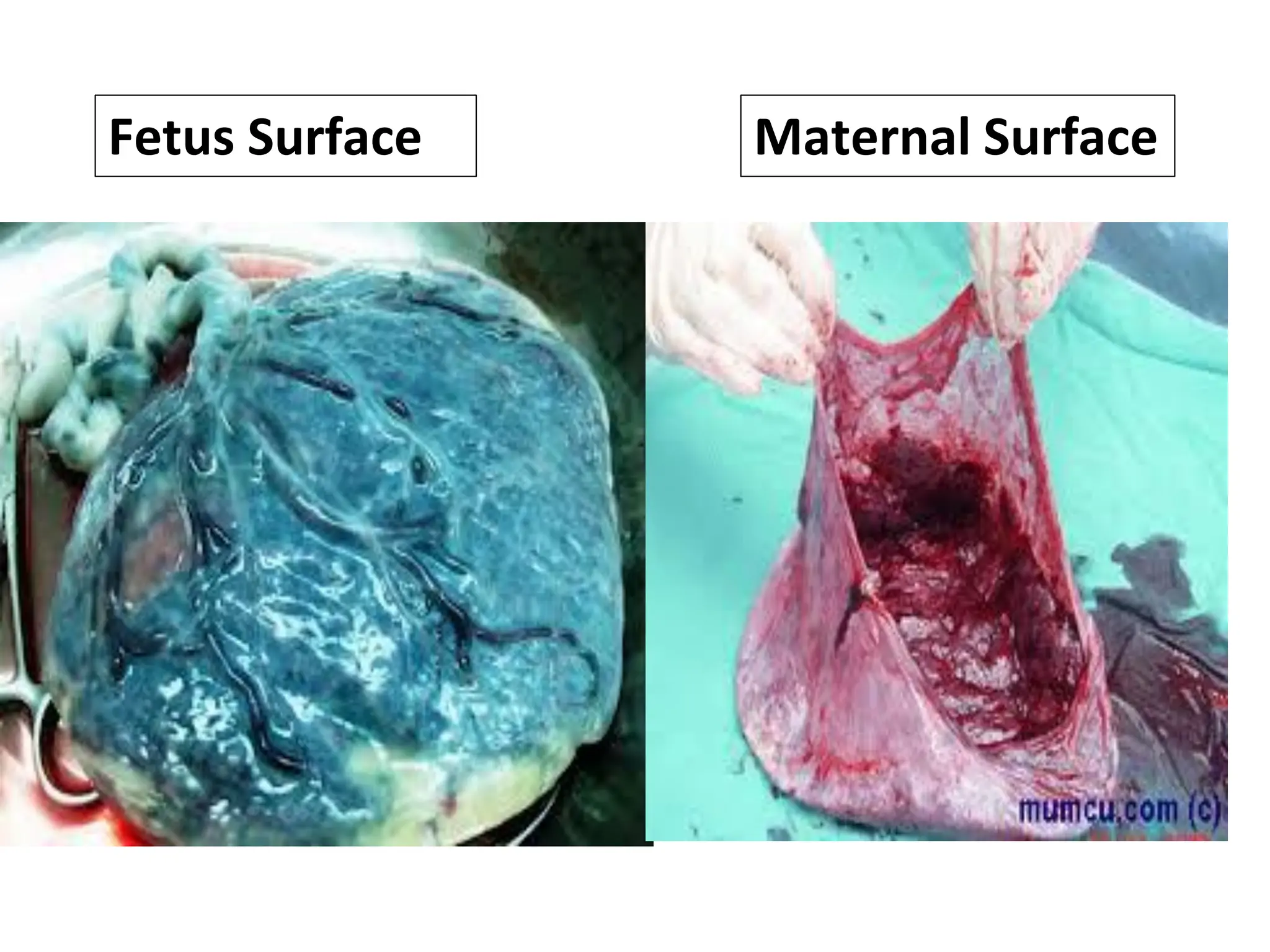
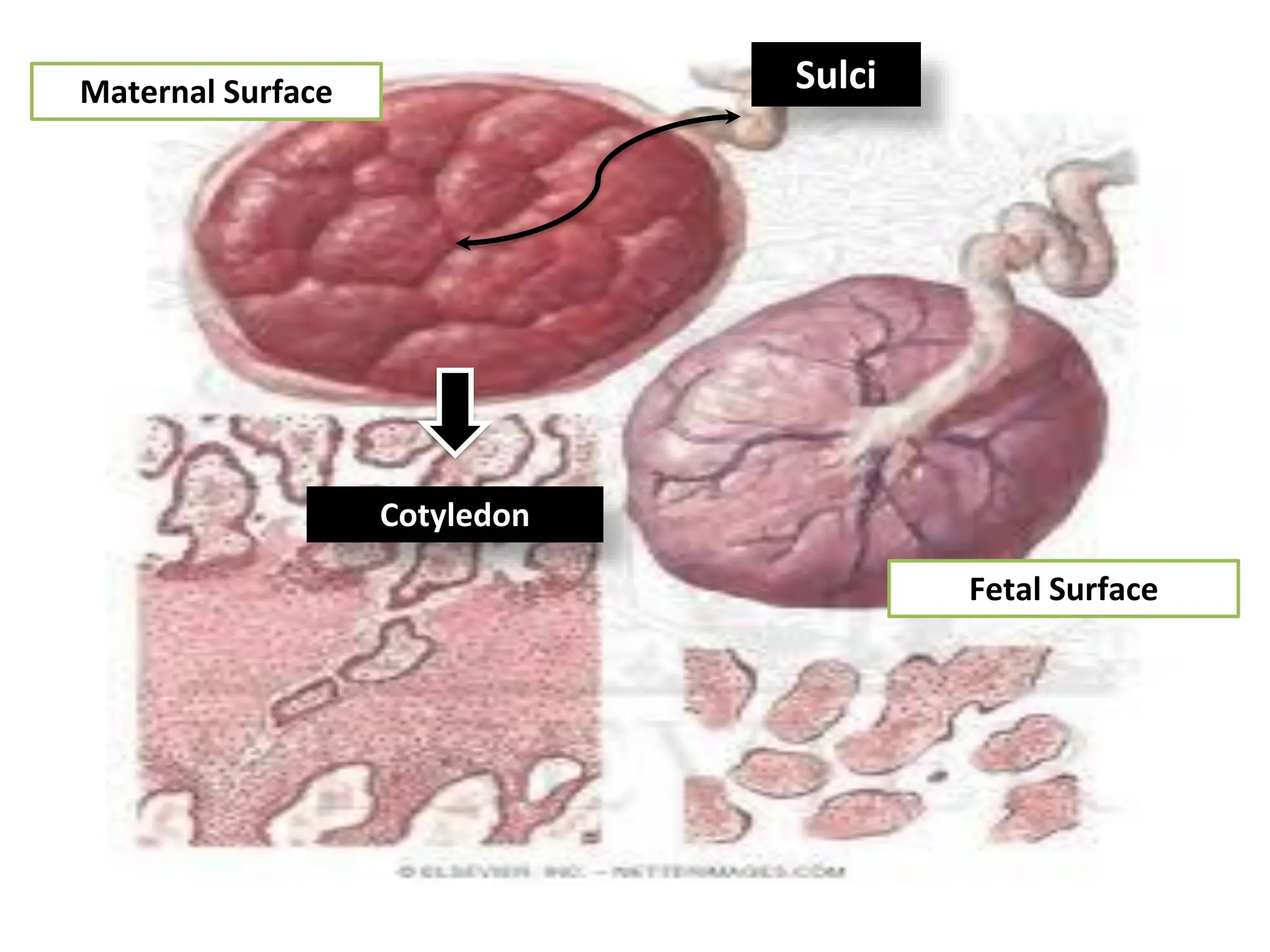
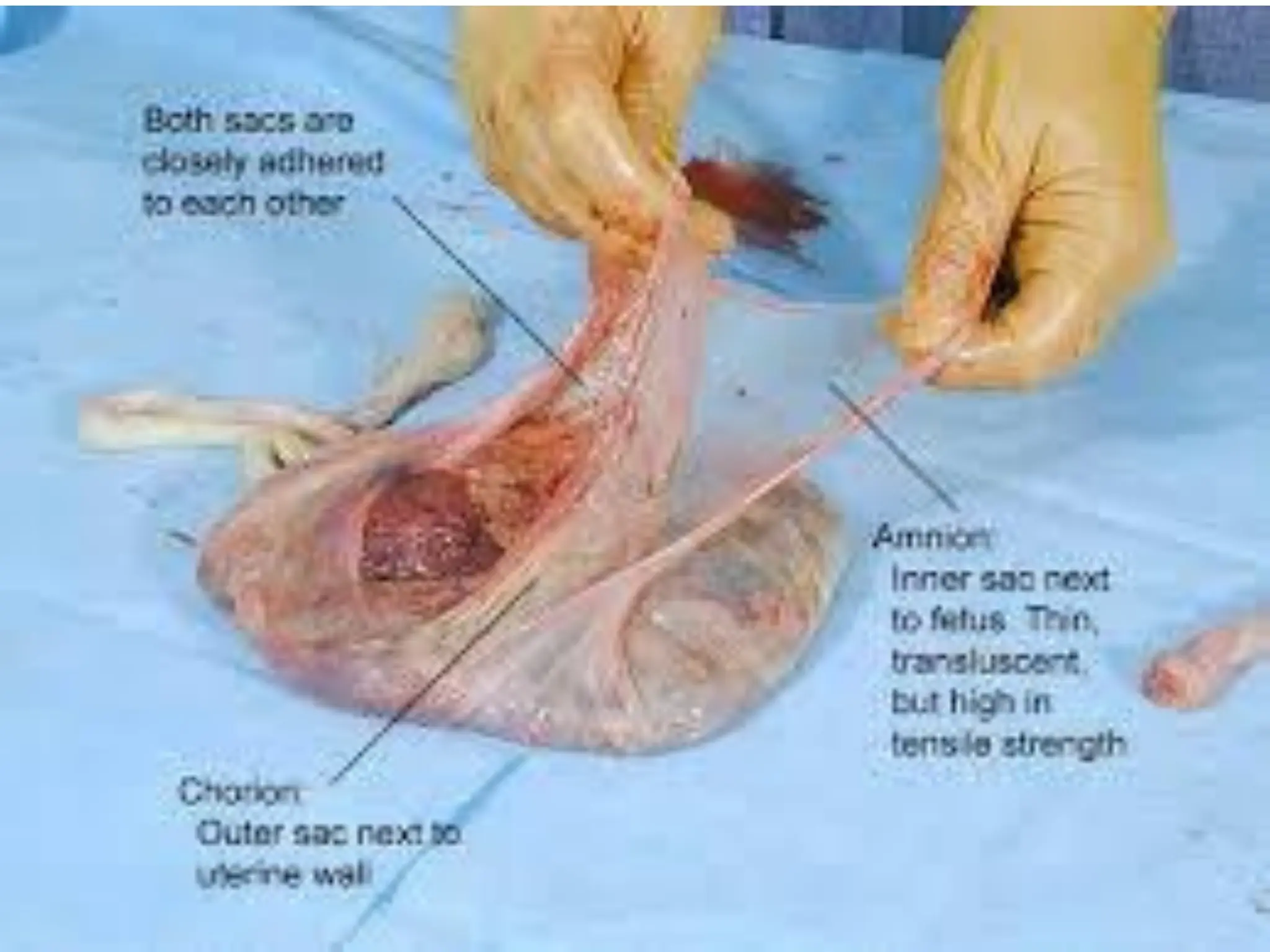
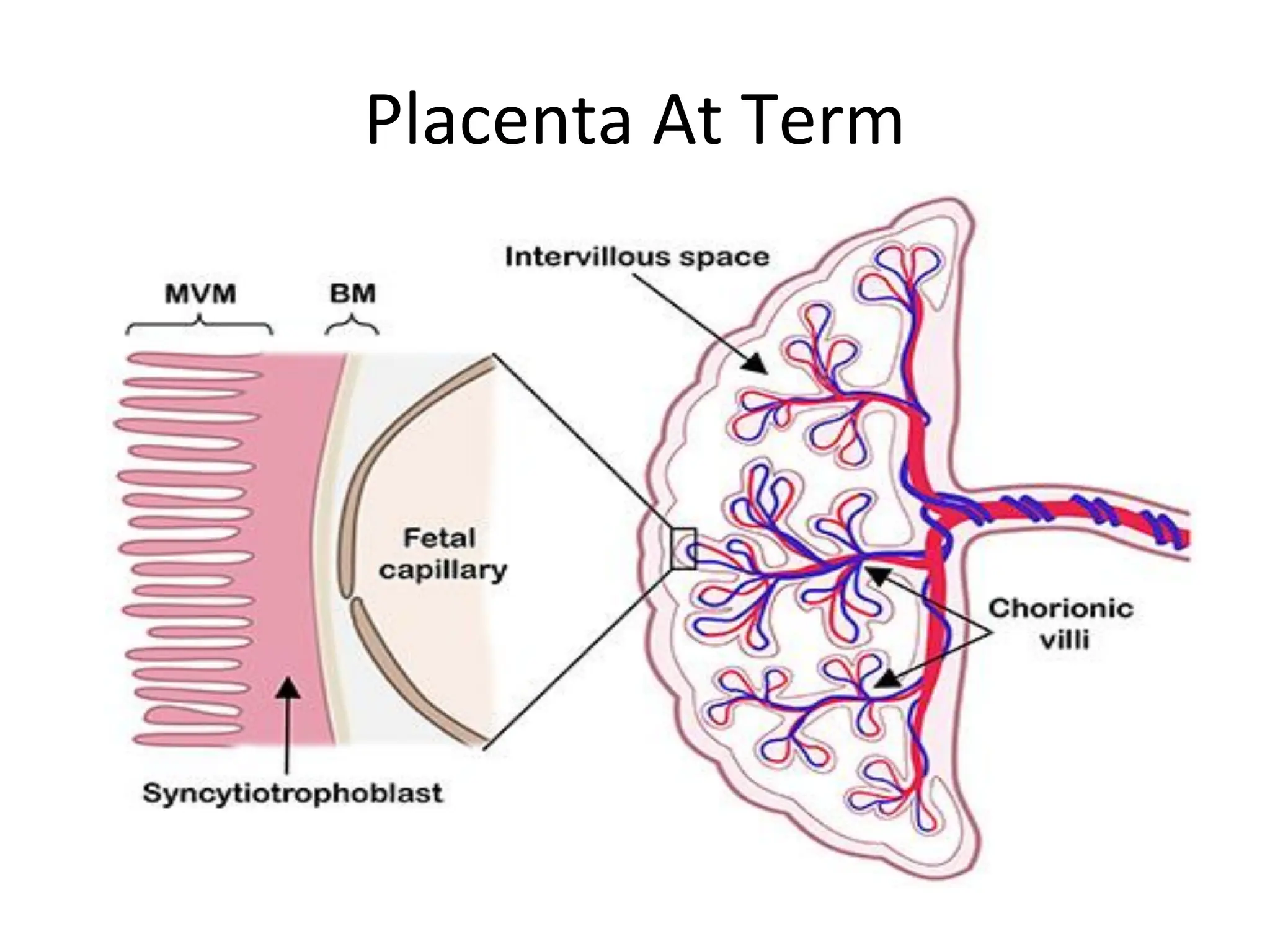
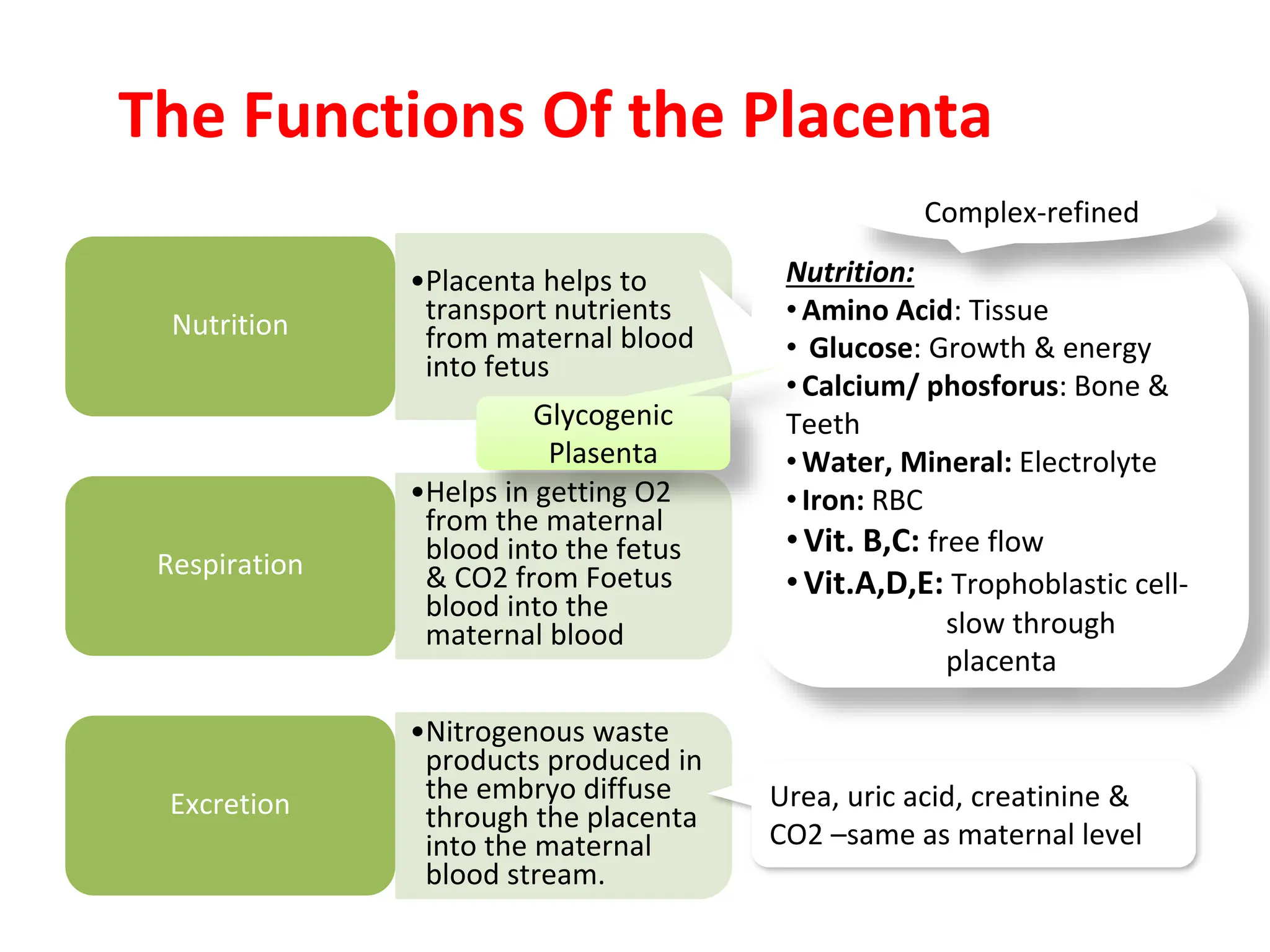
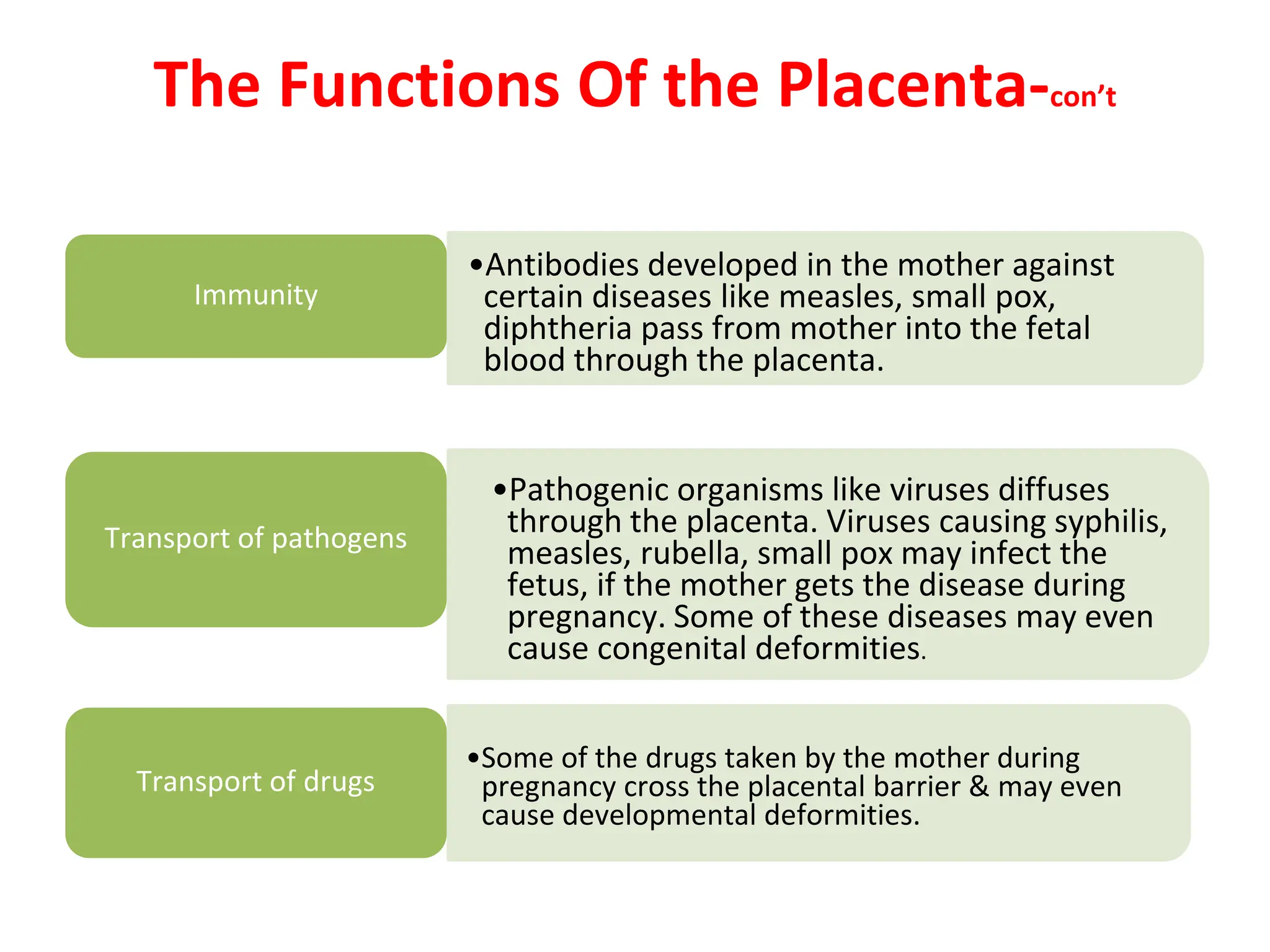
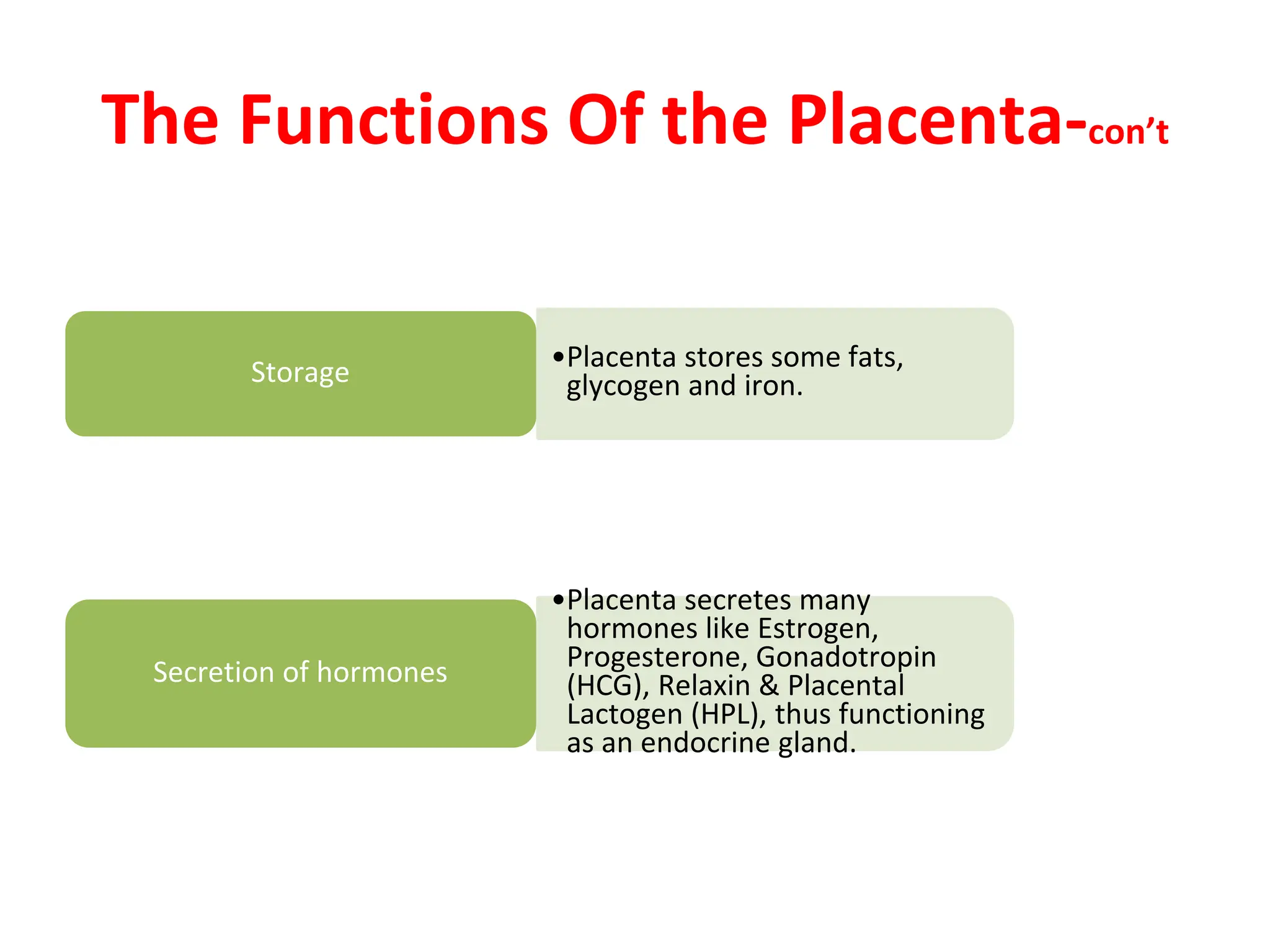
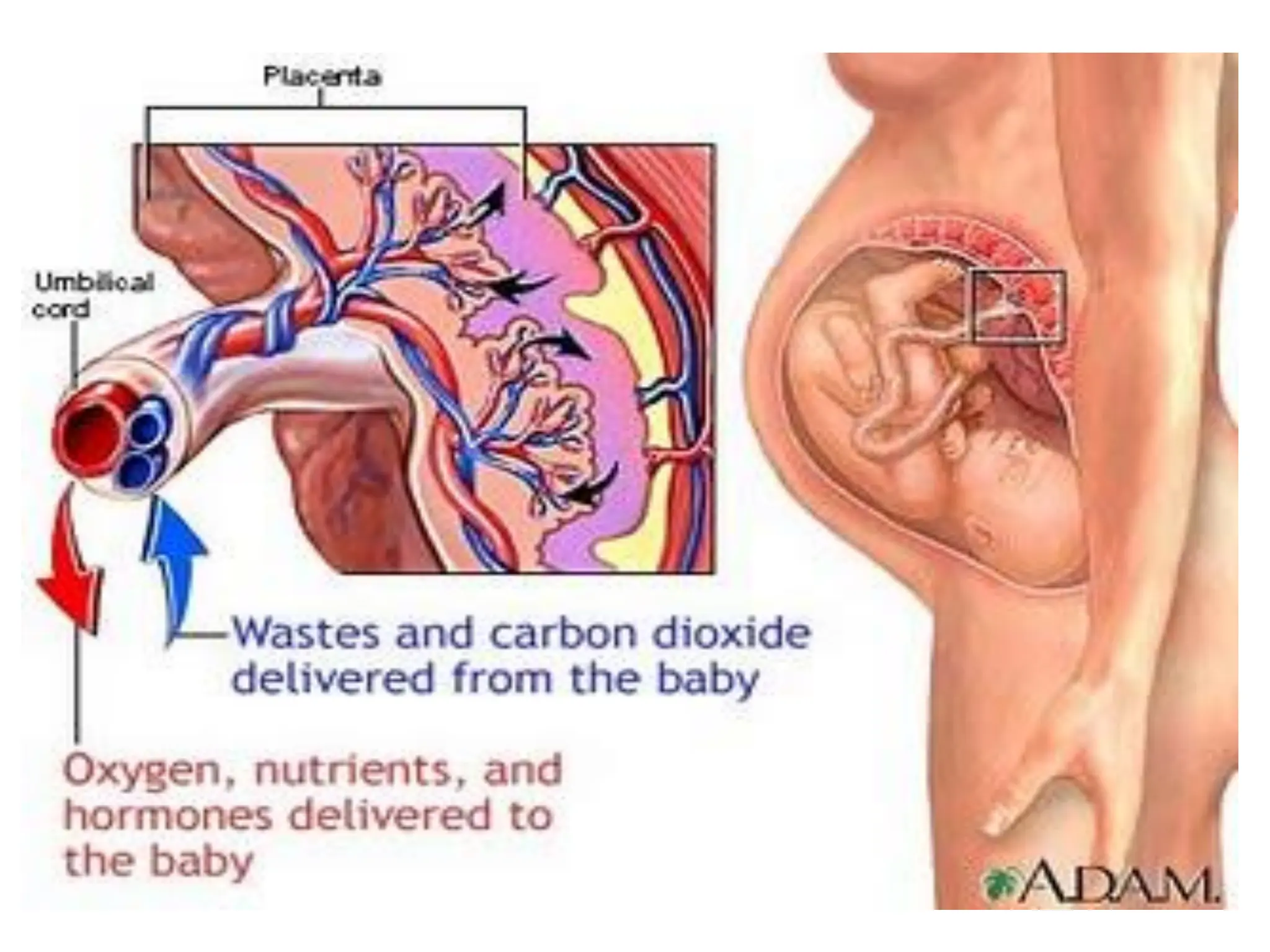
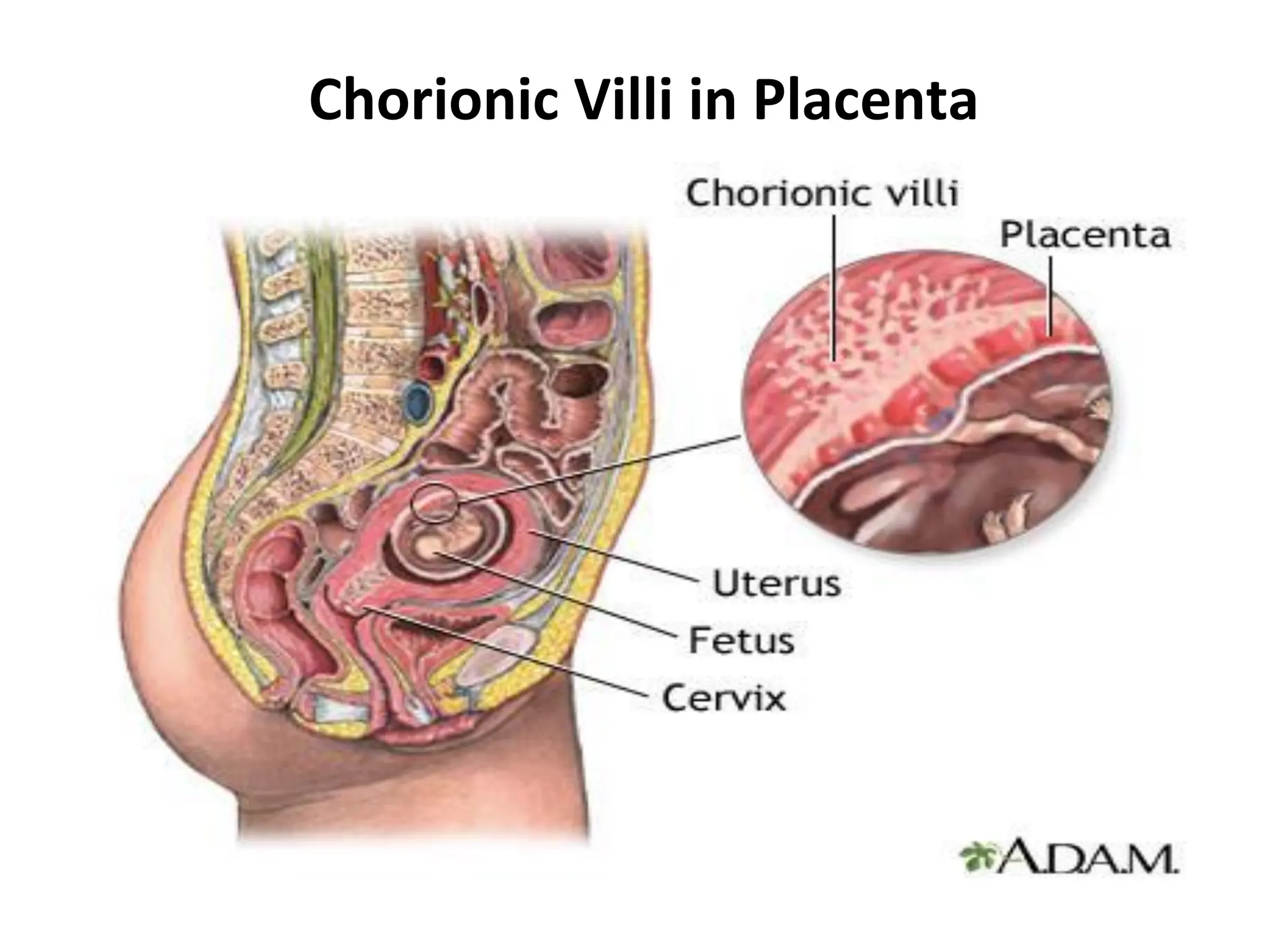
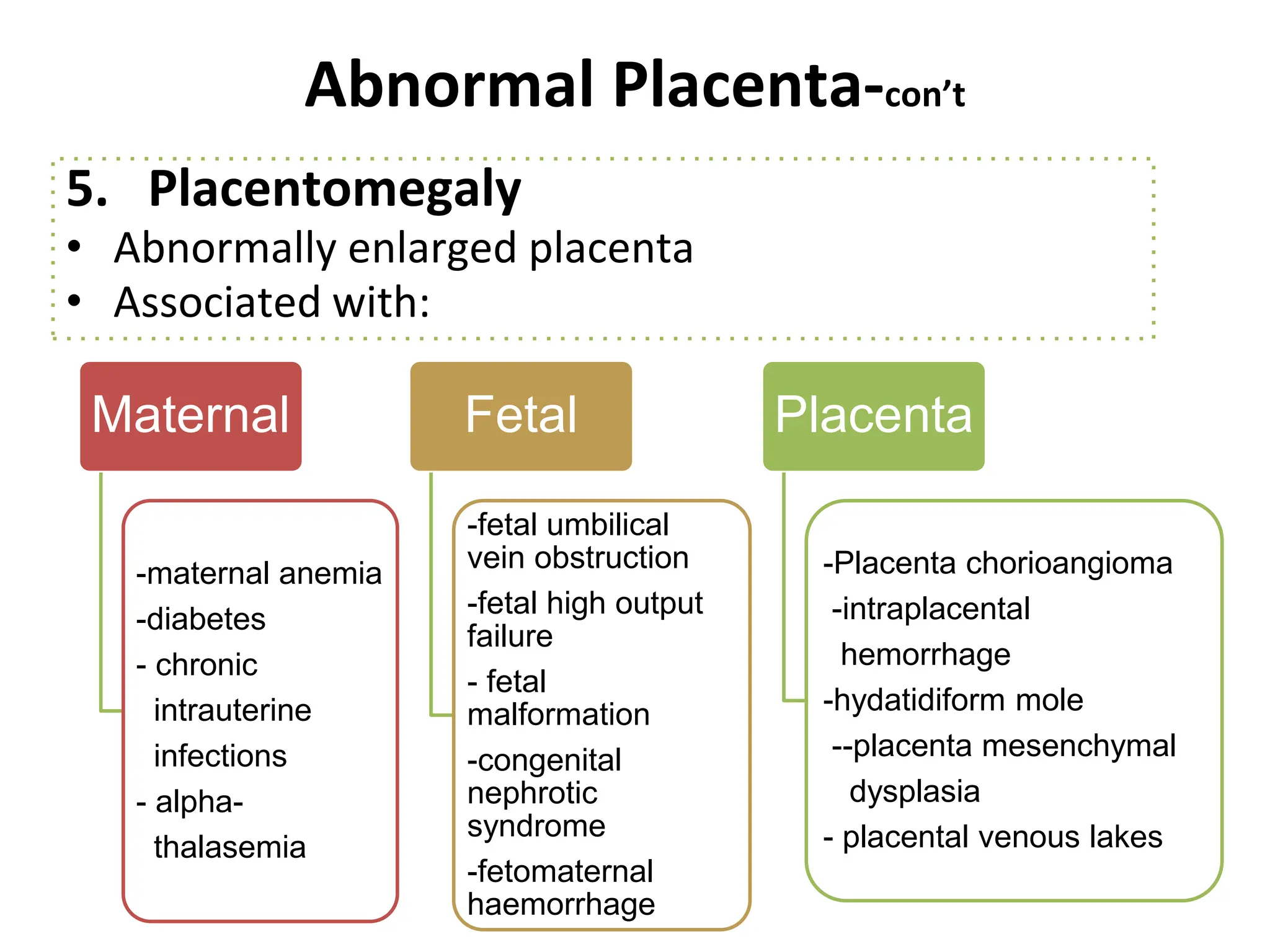
The document discusses the structure and functions of the placenta at term, detailing its gross structure, including the fetal and maternal surfaces, and common abnormalities such as placenta accreta and velamentous insertion. It highlights the placenta's roles in nutrition, respiration, excretion, immunity, drug transport, storage, and hormone secretion. Additionally, it outlines potential dangers posed by abnormalities and various conditions affecting the placenta.