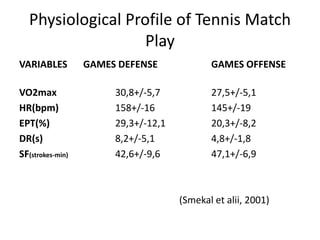

The document outlines the physiological and biomechanical aspects of tennis, emphasizing the importance of strength, endurance, speed, and flexibility in training. It discusses periodization of training cycles and the physiological profile of tennis match play, highlighting factors such as VO2max and lactate concentration. Additionally, it addresses nutritional needs and the risks of overuse injuries, along with strategies for rehabilitation and supplemental training.