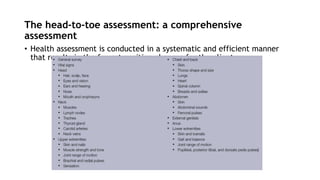
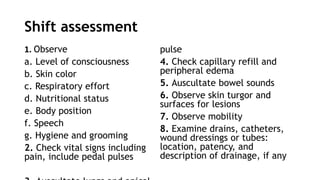
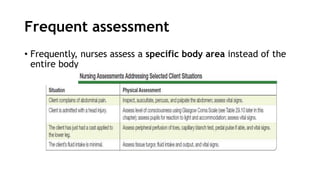
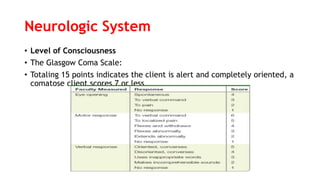
This document provides guidance on conducting a comprehensive physical examination. It outlines the purposes and types of examinations, as well as the techniques used, including inspection, palpation, percussion, and auscultation. It describes how to examine each body system in a systematic manner, from vital signs and general appearance to specific regions like the head, lungs, heart, abdomen, and neurological system. The goal is to assess the client's overall health status and identify any abnormalities through observation, feeling, listening, and other physical assessment methods.