Downloaded 61 times
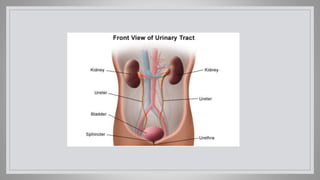
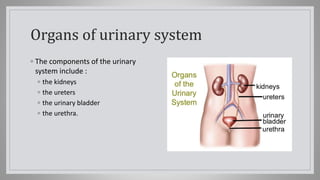
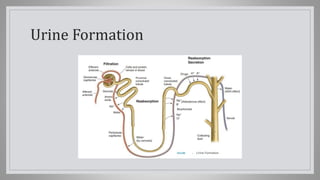

The urinary system consists of the kidneys, ureters, bladder, and urethra, which work together to produce and excrete urine. The kidneys filter waste from the blood to produce urine, which travels through the ureters to the bladder. When full, the bladder empties through the urethra. Urine contains water and waste products like urea, salts, and other dissolved substances. Dysfunctions like incontinence, retention, infection, or changes in urine production can indicate underlying issues.






































![HTHS 1104 Unit 15, Urinary [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hths1104unit15urinaryautosaved-250925164827-104fdfe8-thumbnail.jpg?width=640&height=640&fit=bounds)
















































