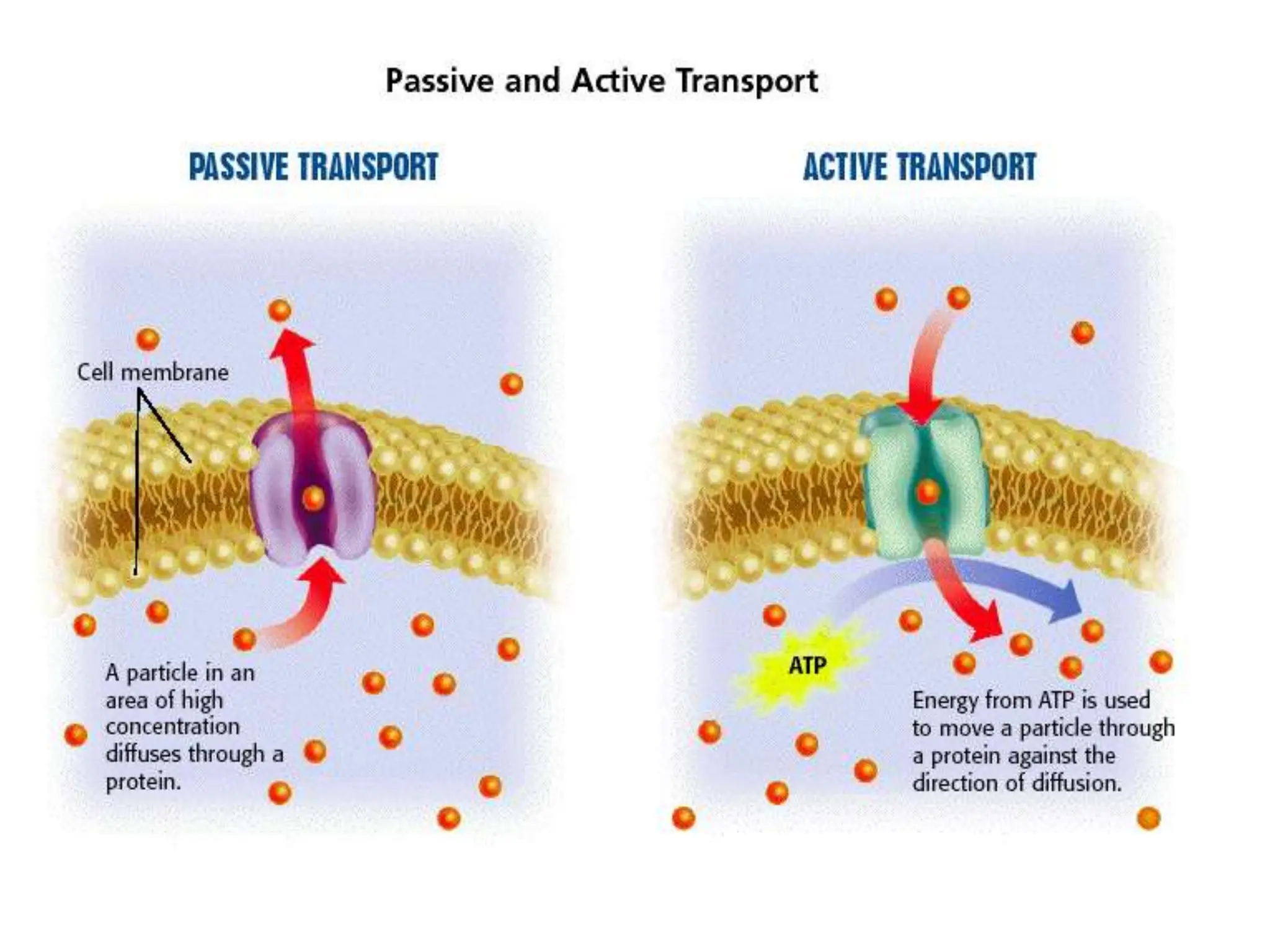
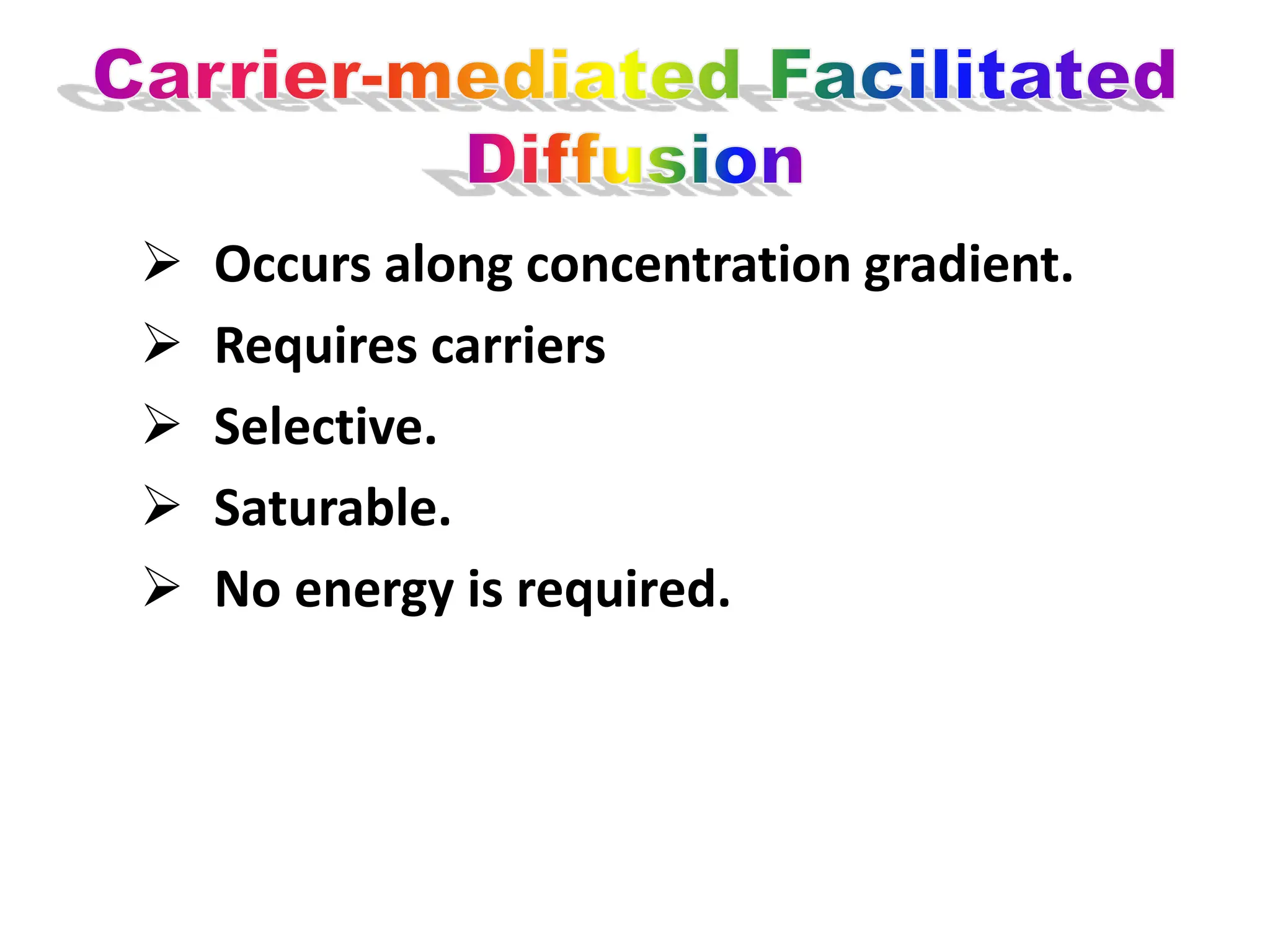
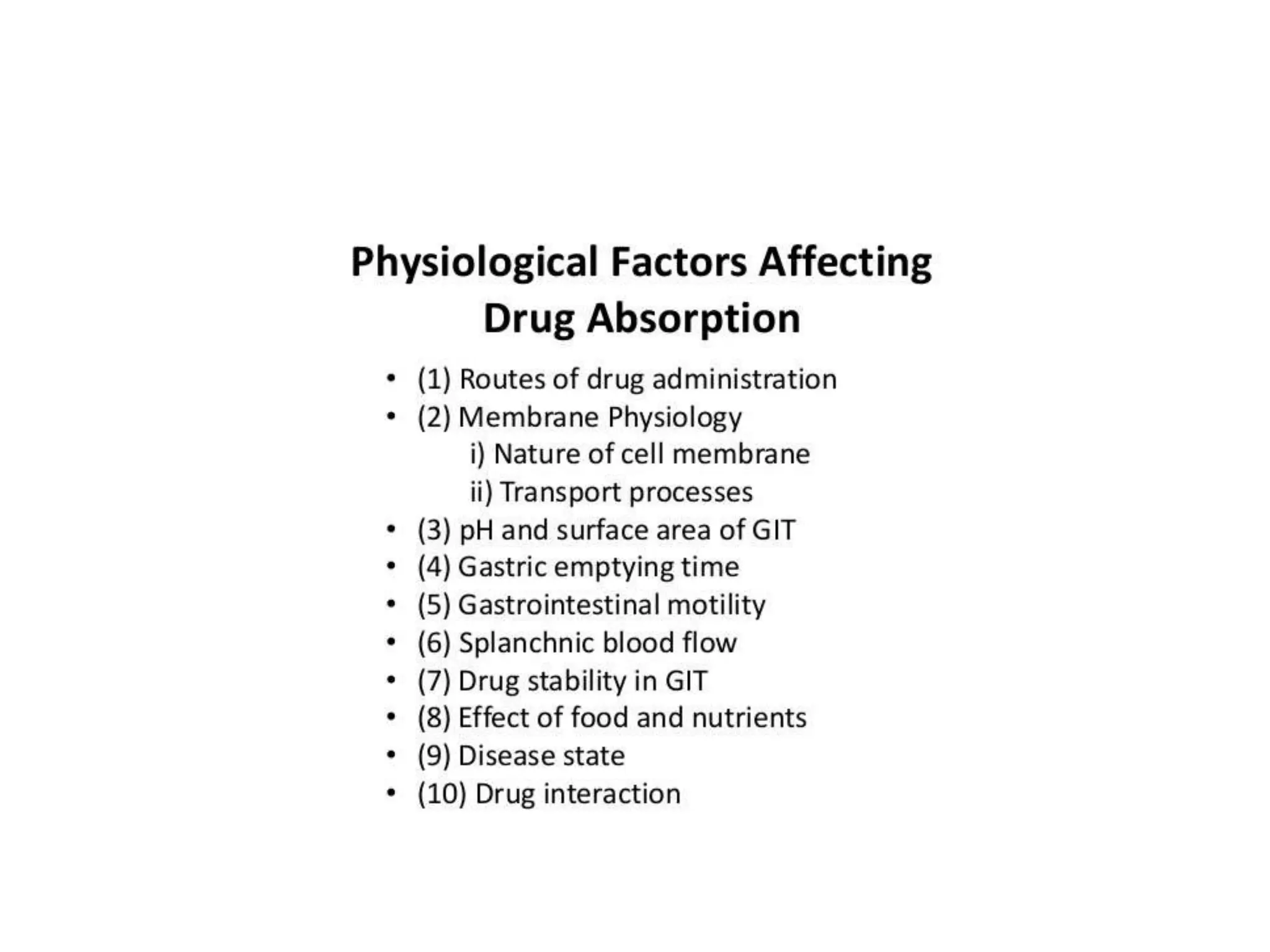
This document provides an overview of pharmacokinetics, specifically focusing on absorption. It defines pharmacokinetics as the study of what the body does to drugs. The four main processes are absorption, distribution, metabolism, and excretion (ADME). Absorption is defined as the passage of drugs through cell membranes to reach the site of action. The main mechanisms of absorption are described as simple diffusion, active transport, facilitated diffusion, and pinocytosis. Factors that influence absorption, such as drug properties and gastrointestinal factors, are also discussed.



































































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)







