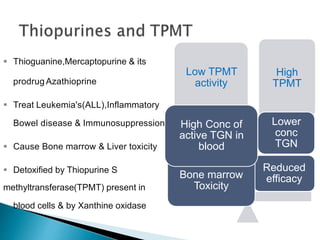
This document discusses pharmacogenetics and how genetic variations can influence individual responses to drugs. It provides definitions and examples of how genes related to drug metabolism and targets can impact drug efficacy and toxicity. Single gene disorders, SNPs, mutations, and inherited conditions are described that influence drug pharmacokinetics and pharmacodynamics. Several clinically applied pharmacogenetic tests are mentioned, such as testing for HLA-B*5701 before prescribing abacavir or DPYD activity before 5-fluorouracil treatment.
























![cmc [ chemistry manufacturing control ]](https://cdn.slidesharecdn.com/ss_thumbnails/presentation2222ra-181120122336-thumbnail.jpg?width=640&height=640&fit=bounds)














































