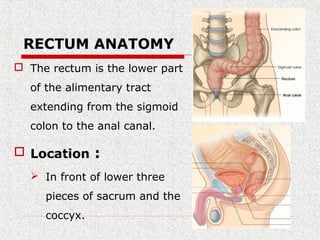
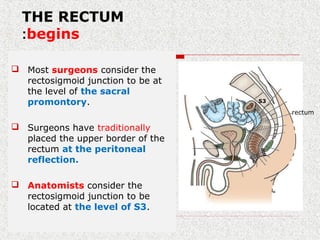
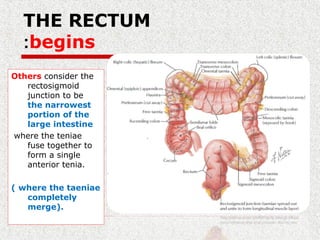
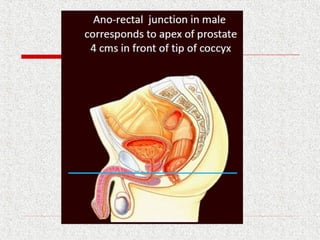
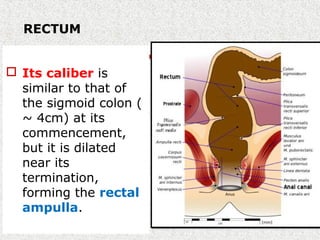
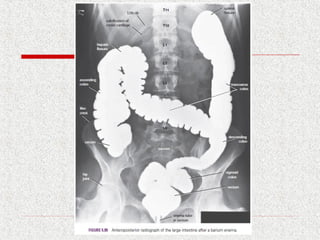
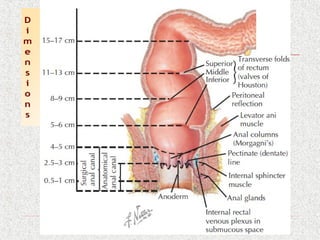
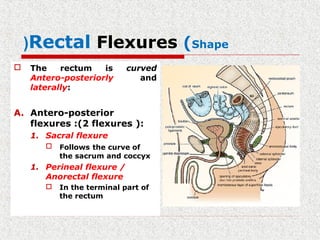
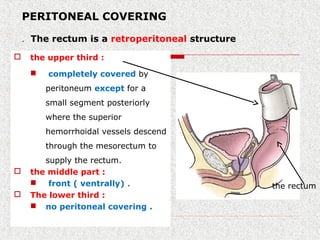
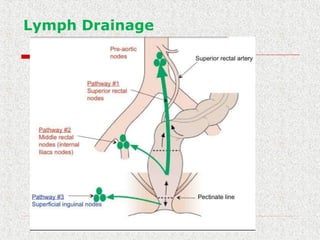
The rectum is the lower part of the large intestine extending from the sigmoid colon to the anal canal. It is around 5 inches long and located in the pelvis in front of the sacrum and coccyx. It has two flexures that follow the curves of the sacrum and coccyx. The upper third is covered in peritoneum while the lower third has no peritoneal covering. It is supplied by branches of the inferior mesenteric artery and drains into internal iliac and inferior mesenteric lymph nodes. A thorough understanding of rectal anatomy is important for surgical management of rectal conditions and cancer.