Download as ODP, PPTX









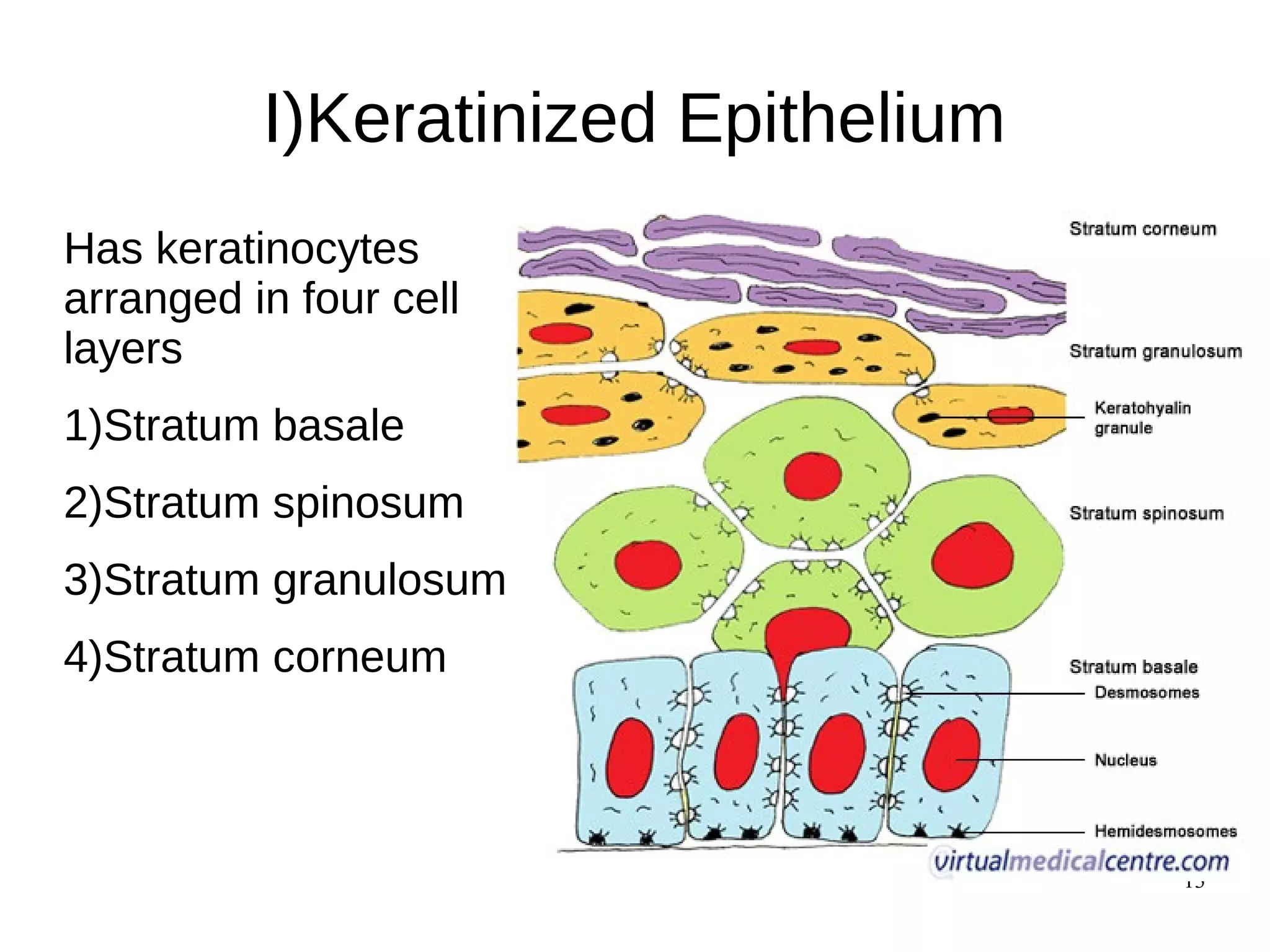




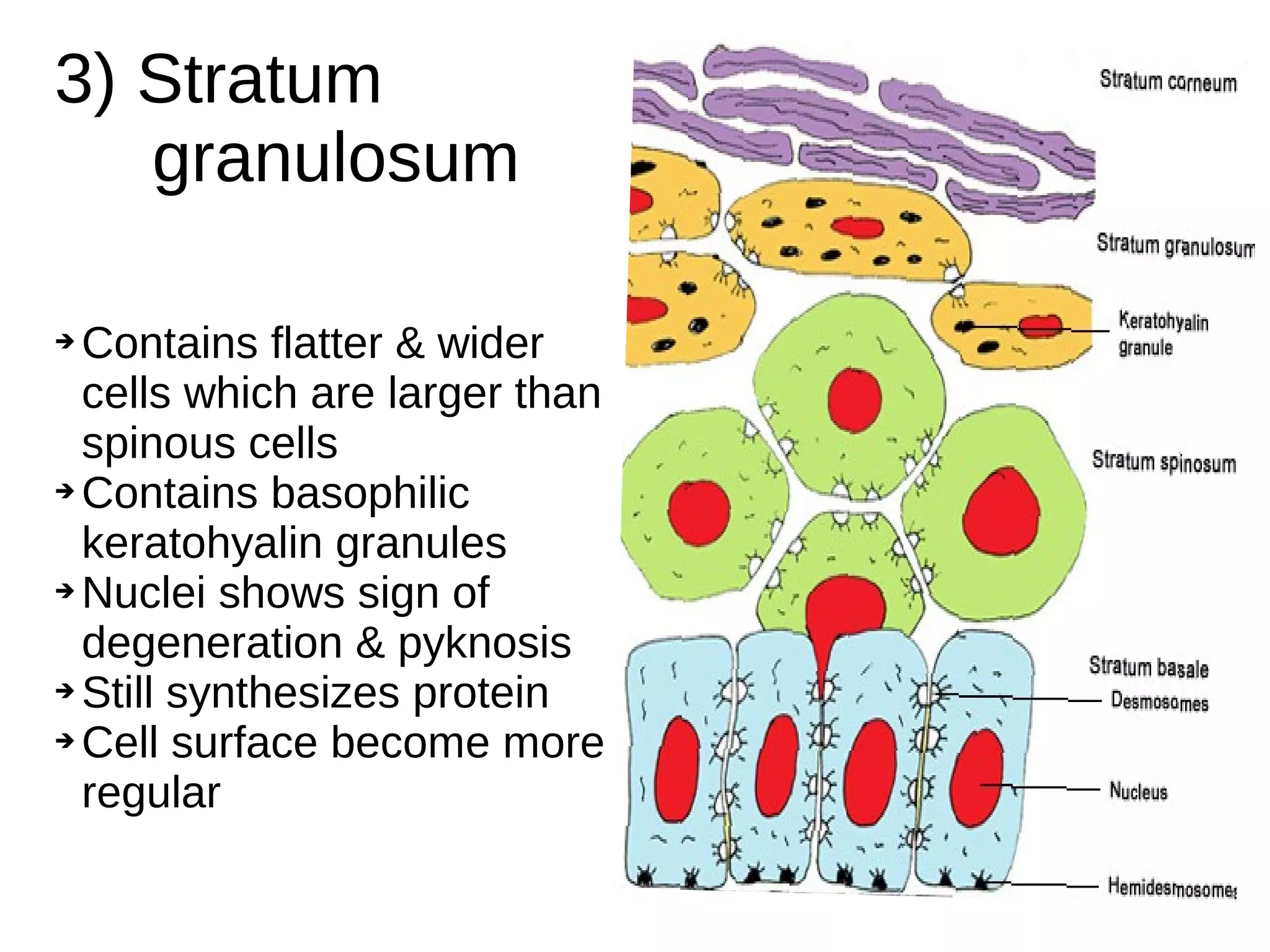









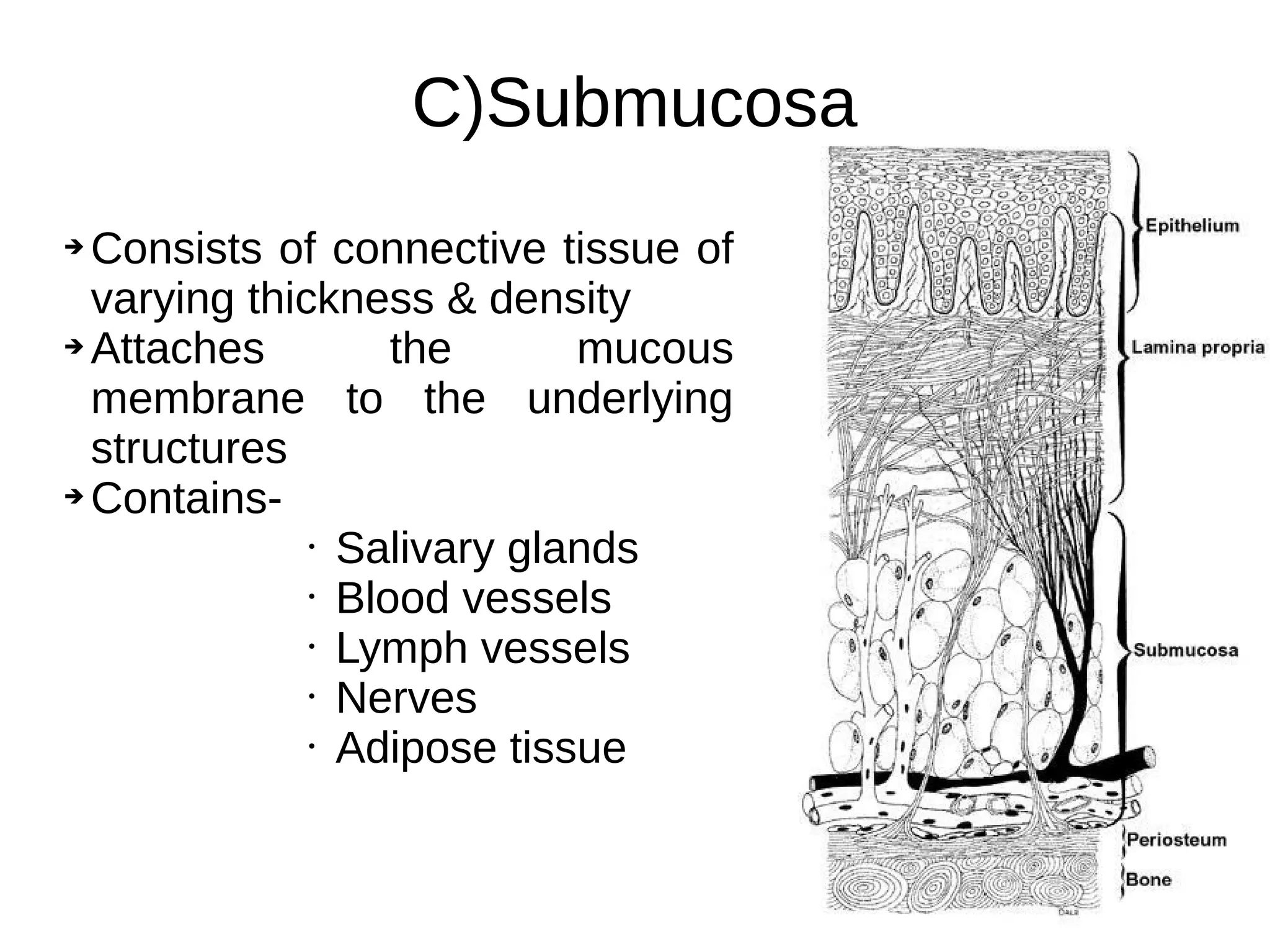
















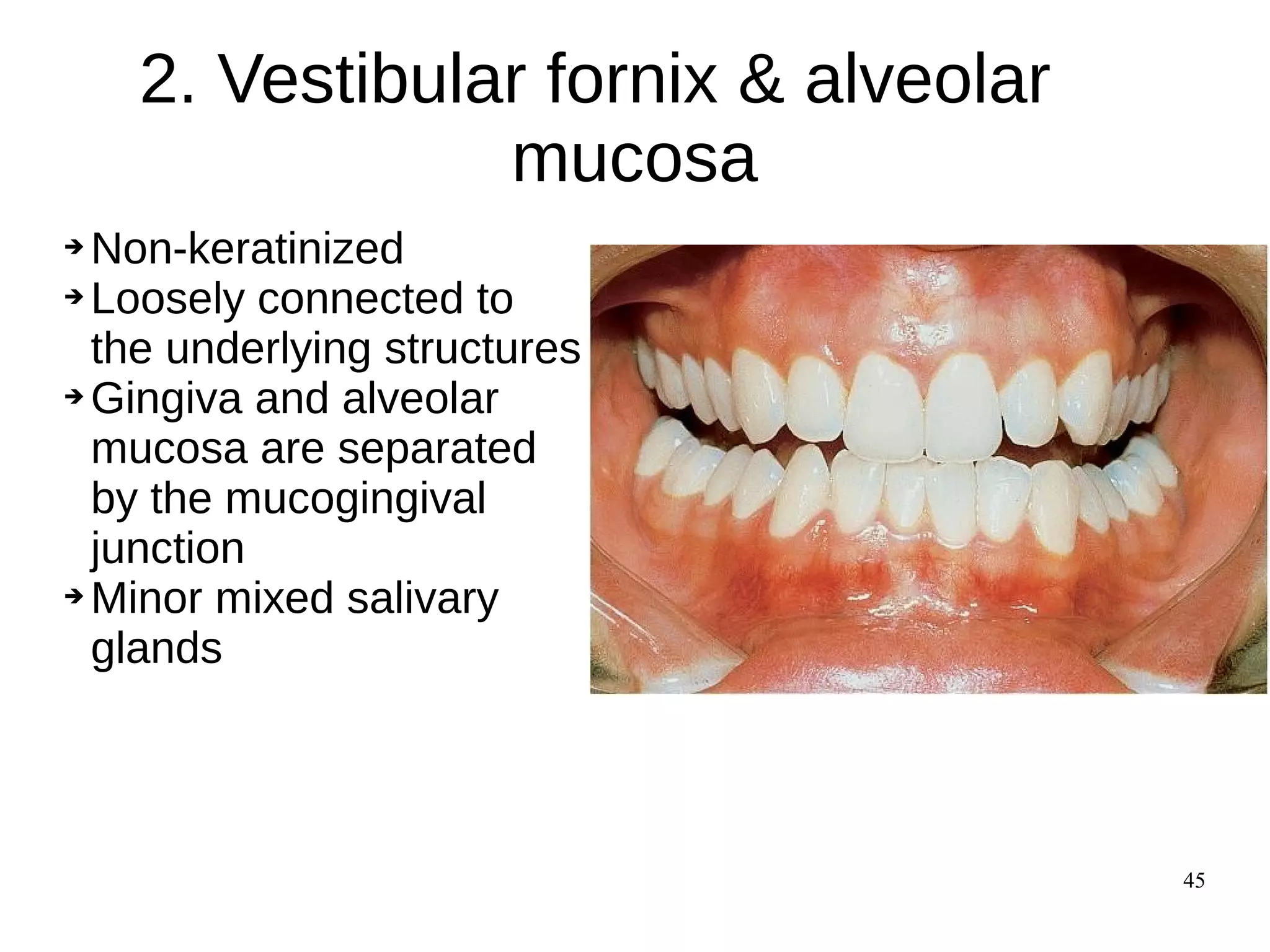



























The document summarizes the histology of oral mucous membrane and its clinical implications. It describes that oral mucosa is classified based on keratinization and location. It has three layers - epithelium, lamina propria, and submucosa. The epithelium can be keratinized or non-keratinized. Keratinized epithelium has four layers while non-keratinized has three layers. Lamina propria contains fibroblasts, collagen and elastic fibers. Submucosa contains salivary glands, blood vessels and nerves. The oral mucosa is subdivided into masticatory, lining and specialized mucosa based on function.



















































































