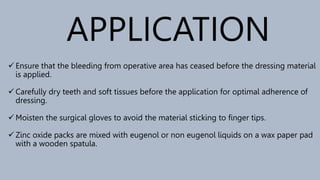
The document provides a comprehensive overview of periodontal dressings, discussing their definitions, rationale for use, ideal properties, types, and application post-surgery. It highlights the ongoing debate over their necessity, mentioning various studies with conflicting evidence regarding their effectiveness and potential drawbacks. Conclusions suggest that the use of dressings is ultimately a matter of patient preference and clinical judgment, specifically for certain surgical procedures.















































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)


