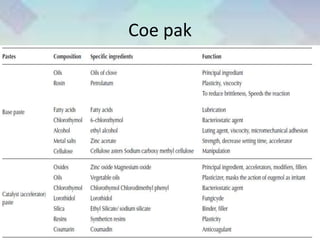
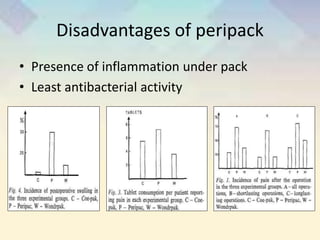
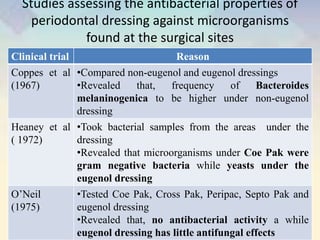
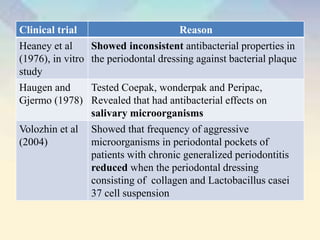
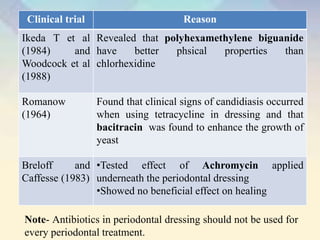
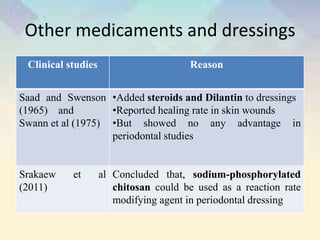
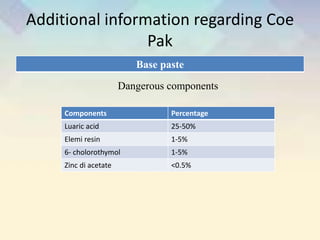
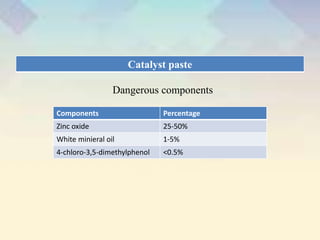
This document provides an overview of periodontal dressings. It discusses the history and evolution of periodontal dressings from early uses of iodoform gauze to modern non-eugenol formulations. The ideal properties and rationale for using periodontal dressings are described. Dressings are classified as those containing zinc oxide and eugenol, zinc oxide without eugenol, or containing neither. Specific dressing formulations including Coe-Pak, Cross-Pak, Peripac, and Septo-Pack are outlined detailing their compositions, properties, and uses.