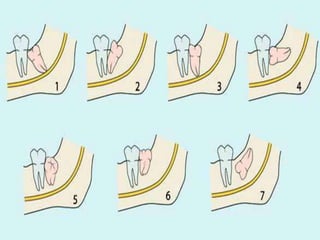
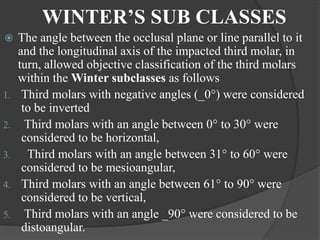
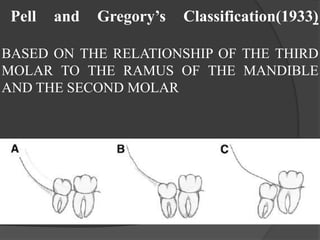
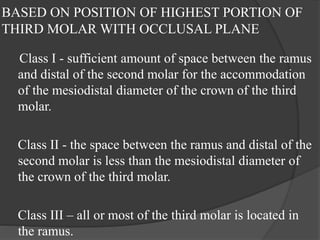
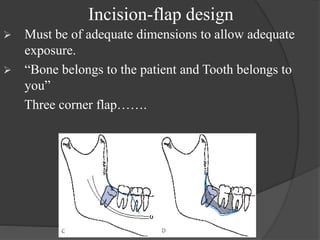
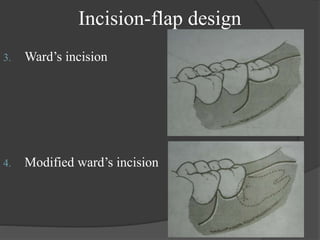
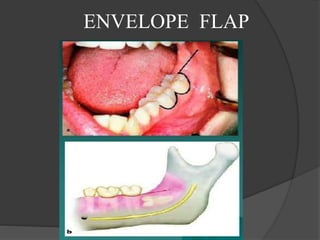
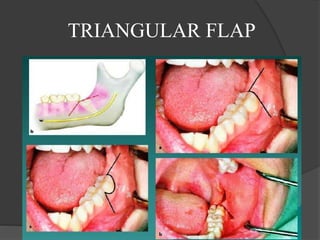
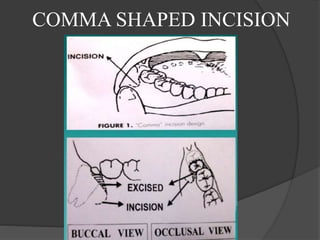
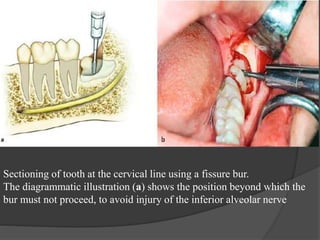
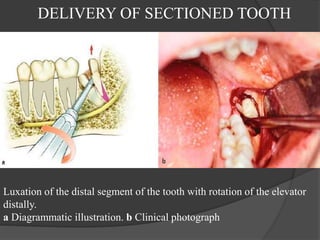
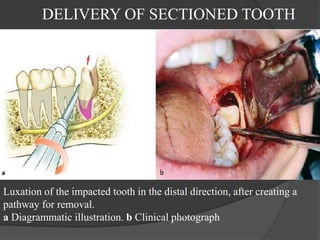
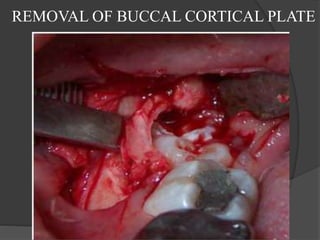
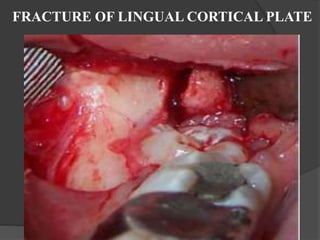
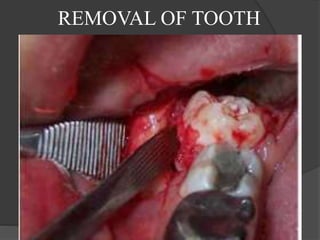
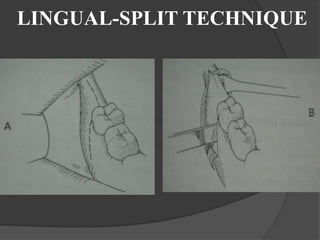
This document provides information on impacted third molars and their surgical removal. It begins with definitions of impacted and unerupted teeth. It then discusses the various classifications of impacted third molars based on their position, such as Winter's classification. The document outlines the surgical procedure for removal, including flap design, bone removal, tooth sectioning if needed, and delivery of the impacted tooth. It emphasizes performing the surgery in an aseptic manner to minimize complications.