Downloaded 13 times

![Adapted from Mozes G, Gloviczki P: Vasc Endovasc Surg 2004;38:367-74.
great
Mendoza et al. (eds.), Duplex Ultrasound of Superfi cial Leg Veins, 19 731-4_2, © Springer-Verlag Berlin Heidelberg
2014]
CLINICALLY RELEVANT PERFORATORS, POSTERIOR LEG:](https://image.slidesharecdn.com/perforatorphysiciantrainingarbid-210423151113/85/Perforator-physician-training-arbid-10-320.jpg)
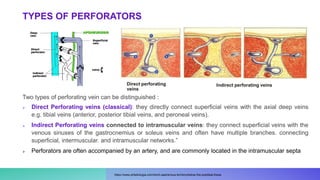
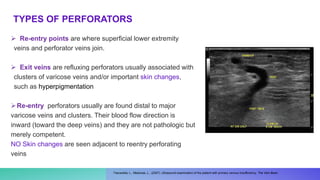
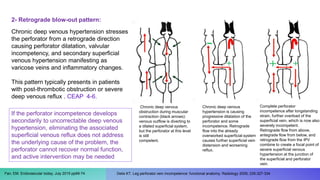
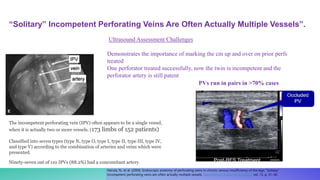
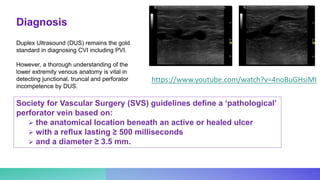



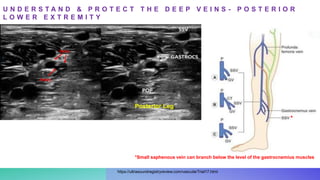
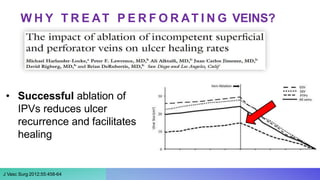


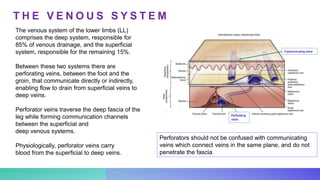
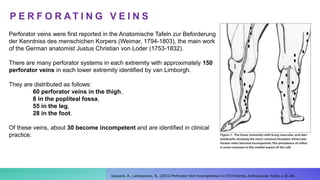
Perforating veins connect the superficial and deep venous systems of the legs, allowing blood flow between the two. They are normally competent, only allowing flow from superficial to deep veins. Incompetence can develop through two mechanisms: (1) antegrade overload from superficial reflux overworking perforators, or (2) retrograde overload from deep venous hypertension blowing out perforators from below. Incompetent perforators are associated with worsening venous disease and often need treatment. Ultrasound assessment of perforators can be challenging as they frequently occur in pairs or groups rather than individually.



































































