
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Parkinsons disease
Similar to Parkinsons disease (20)
More from sai kiran Neeli
Recently uploaded
Recently uploaded (20)
Parkinsons disease
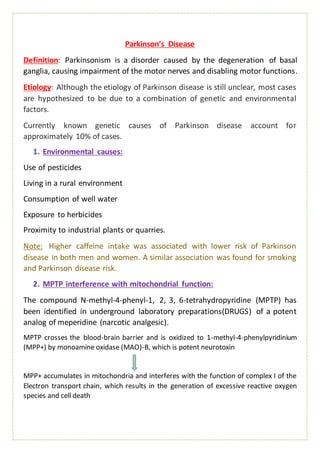
- 1. Parkinson’s Disease Definition: Parkinsonism is a disorder caused by the degeneration of basal ganglia, causing impairment of the motor nerves and disabling motor functions. Etiology: Although the etiology of Parkinson disease is still unclear, most cases are hypothesized to be due to a combination of genetic and environmental factors. Currently known genetic causes of Parkinson disease account for approximately 10% of cases. 1. Environmental causes: Use of pesticides Living in a rural environment Consumption of well water Exposure to herbicides Proximity to industrial plants or quarries. Note: Higher caffeine intake was associated with lower risk of Parkinson disease in both men and women. A similar association was found for smoking and Parkinson disease risk. 2. MPTP interference with mitochondrial function: The compound N-methyl-4-phenyl-1, 2, 3, 6-tetrahydropyridine (MPTP) has been identified in underground laboratory preparations(DRUGS) of a potent analog of meperidine (narcotic analgesic). MPTP crosses the blood-brain barrier and is oxidized to 1-methyl-4-phenylpyridinium (MPP+) by monoamine oxidase (MAO)-B, which is potent neurotoxin MPP+ accumulates in mitochondria and interferes with the function of complex I of the Electron transport chain, which results in the generation of excessive reactive oxygen species and cell death
- 2. 3. Oxidation hypothesis: The oxidative metabolism of dopamine by MAO-B leads to the formation of hydrogen peroxide. Normally, hydrogen peroxide is cleared rapidly by glutathione, but if hydrogen peroxide is not cleared adequately, it may lead to the formation of highly reactive hydroxyl radicals that can react with cell membrane lipids to cause lipid peroxidation and cell damage. In Parkinson disease, levels of reduced glutathione are decreased, suggesting a loss of protection against formation of free radicals. Iron is increased in the substantia nigra and may serve as a source of donor electrons, thereby promoting the formation of free radicals. 4. Genetic factors: Genetics may play a significant role, particularly if PD begins before age 50 years. Autosomal dominant forms of parkinsonism are associated with mutations of the α-synuclein (PARK1 and PARK4) and leucine-rich repeat kinase 2 (LRRK) genes. Autosomal recessive forms are associated with mutations of parkin (PARK2) and PTEN-induced putative kinase 1 (PINK1) genes (DOPAC- 3,4- dihydroxyphenyl aceticacid; GSH- glutathione; GSSG-glutathione disulfide
- 3. Mechanisms related to genes- abnormal protein aggregation (alpha-synuclein), defective ubiquitin-mediated protein degradation of alpha-synuclein, mitochondrial dysfunction, and oxidative damage. 5. Alpha-synuclein conformational changes and aggregation: Normally, alpha-synuclein is found mainly in neuronal presynaptic terminals and may play a role in assembly and function of SNARE (soluble N- ethylmaleimide-sensitive factor activating protein receptor) proteins that are involved in neurotransmitter release. Under certain conditions (genetic mutations), alpha-synuclein aggregates into oligomers that are gradually converted to the beta–sheet-rich fibrillary structures that form Lewy bodies and neurites in Parkinson disease. i. oligomeric alpha-synuclein can promote formation of ion-permeable pores on neuronal membranes, leading to increased calcium influx. ii. Aberrant pore formation could also lead to neurotransmitter leaks from synaptic vesicles into the cytosol. iii. oligomeric alpha-synuclein may have a direct effect on mitochondrial membranes. iv. oligomerization of alpha-synuclein could cause cytoskeletal disruption, possibly by an effect on the microtubule-stabilizing protein, tau. 6. Melanoma 7. Diabetes Pathophysiology: The 2 major neuropathologic findings in Parkinson disease are: i. Loss of pigmented dopaminergic neurons of the substantia nigra pars compacta ii. The presence of Lewy bodies and Lewy neurites (alpha-synuclein)
- 4. Etiological factors Dopaminergic neurons in substantia nigra starts to die of (Nigrostriatal pathway) i. It cannot initiate more movements in Direct pathway ii. It cannot prevent excessive reduction in movement in the Indirect pathway Slowing down and Loss of movements Motor control by basal ganglia
- 5. Signs and symptoms: General Features Common early motor signs of Parkinson disease include resting tremor, rigidity, or bradykinesia. Postural instability (difficulty with maintaining balance) is more common in advanced IPD. Motor Symptoms The patient experiences: i. Decreased manual dexterity (ability to use your hands in a skillful, coordinated way to grasp and manipulate objects and demonstrate small, precise movements), ii. Difficulty arising from a seated position, iii. Diminished arm swing during ambulation (ability to walk without the need for any kind of assistance), iv. Dysarthria (slurred speech), v. Dysphagia (difficulty with swallowing), vi. Festinating gait (tendency to pass from a walking to a running pace), vii. Flexed posture (axial, upper/lower extremities), viii. “freezing” at initiation of movement, ix. Hypomimia (reduced facial animation), x. Hypophonia (reduced voice volume), and xi. Micrographia (diminution of handwritten letters/symbols) Autonomic and Sensory Symptoms i. The patient experiences: ii. Bladder and anal sphincter disturbances, iii. Constipation, iv. Diaphoresis, v. Fatigue, vi. Olfactory disturbance, vii. Orthostatic blood pressure changes, viii. Pain, paresthesia, ix. Paroxysmal vascular flushing, seborrhea, sexual dysfunction, and sialorrhea (drooling).
- 6. Mental Status Changes The patient experiences: i. Anxiety, ii. Apathy, iii. Bradyphrenia (slowness of thought processes), iv. Confusional state, v. Dementia, vi. Depression, vii. Hallucinosis/psychosis (typically drug induced), and viii. Sleep disorders (excessive daytime sleepiness, insomnia, obstructive sleep apnea, and rapid eye movement sleep behavior disorder). Diagnosis: No laboratory tests are available to diagnose PD Genetic testing is not routinely helpful. Neuroimaging may be useful for excluding other diagnoses. Medication history should be obtained to rule out drug induced parkinsonism. Treatment: Goals: The goal in the management of PD is To improve motor and nonmotor symptoms so that patients are able to maintain the best possible quality of life. Specific objectives to consider when selecting an intervention include preservation of the ability to perform activities of daily living; improvement of mobility; minimization of adverse effects, treatment complications; and improvement of nonmotor features such as cognitive impairment, depression, fatigue, and sleep disorders.
- 7. General approach tothe management of early to advancedParkinson’s disease.
- 9. Drugs and their site of Action Further Info about drugs in Pharmacology material…