Downloaded 42 times

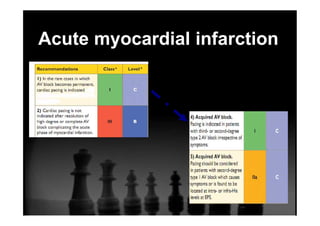
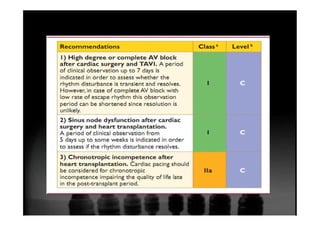
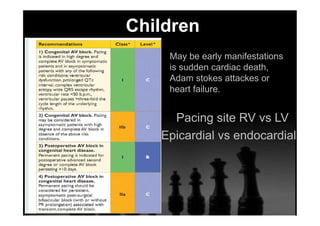
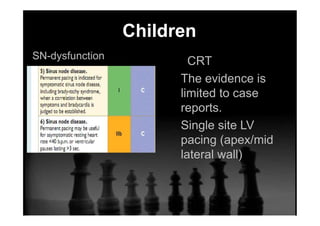
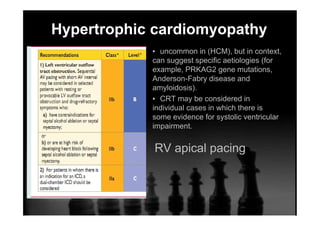

The document outlines updated guidelines for pacing in various special conditions, including acute myocardial infarction, cardiac surgery, congenital heart disease, and pregnancy. It discusses the incidence and management of AV blocks post-procedures, indicating a need for observation before permanent pacing in certain cases. Additionally, it highlights specific pacing strategies and considerations in children and those with rare diseases, with a focus on tailored approaches based on individual patient circumstances.









































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)













