Downloaded 86 times

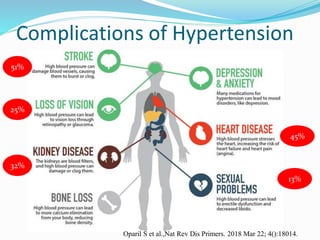
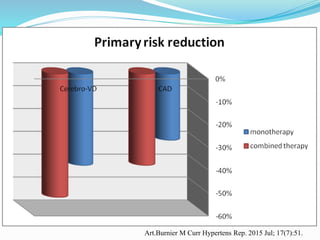
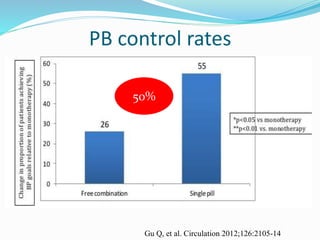
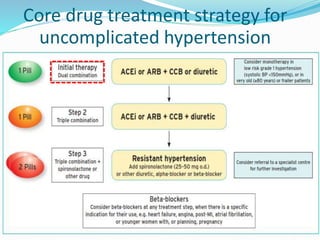
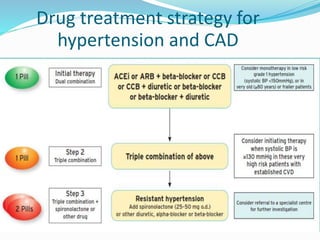
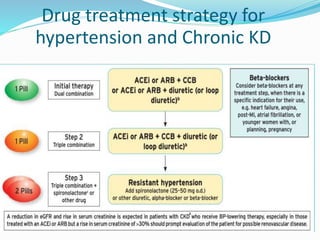
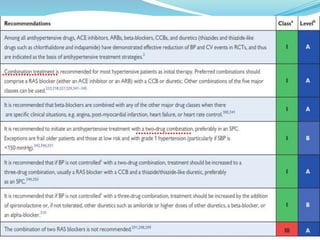
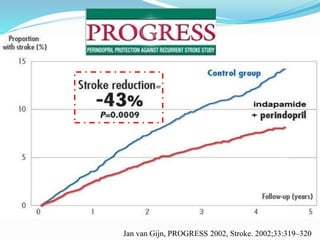
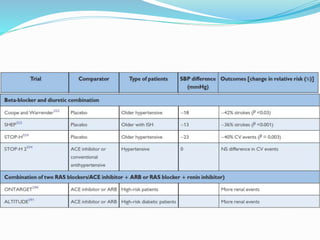
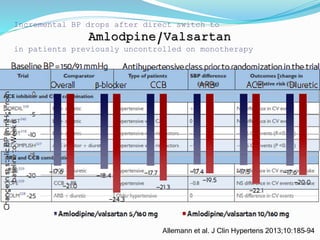
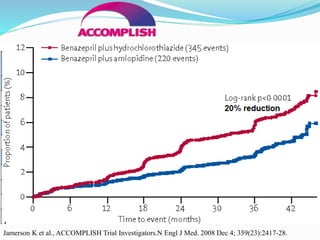



Initial combination therapy is superior to sequential mono-therapy for treating hypertension. Combination therapy controls blood pressure faster by acting on multiple mechanisms, reducing complications by 40-54%. Combinations have greater efficacy, improve adherence, and have protective effects beyond blood pressure lowering like anti-inflammatory and metabolic benefits. Clinical trials show combination therapy achieves better blood pressure control rates and lowers cardiovascular events compared to mono-therapy. Therefore, guidelines recommend starting treatment for hypertension with initial combination therapy.























































































