Download as PDF, PPTX














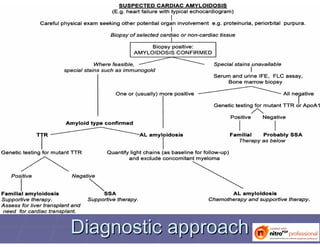
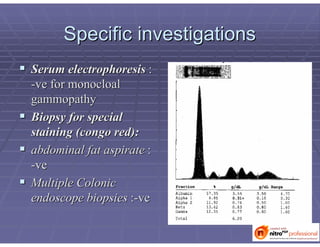



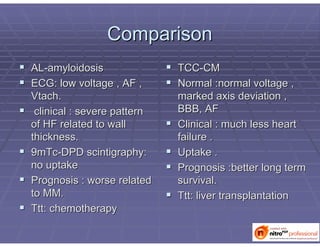
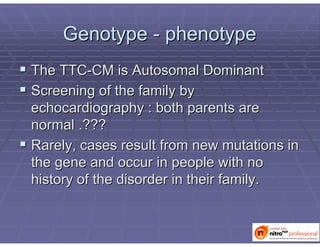




This document discusses the case of a 23-year-old male patient who presented with dyspnea and chest pain. After extensive testing and examination, he was diagnosed with transthyretin cardiac amyloidosis (TTR-CM), a rare hereditary form of amyloidosis. The document compares TTR-CM to other types of amyloidosis and discusses the patient's family history, treatment options, and prognosis. Tissue Doppler imaging and biopsy were important for confirming the diagnosis. While rare, this case demonstrates that TTR-CM can still occur and requires an integrated approach to diagnose.




























































































