Downloaded 17 times

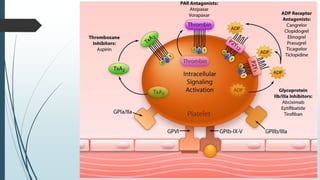
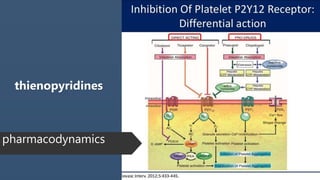
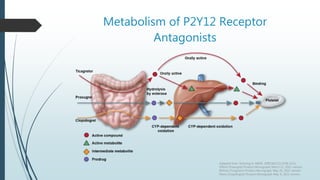
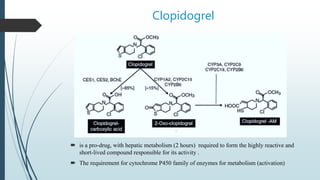
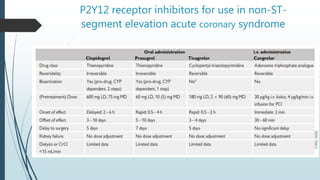

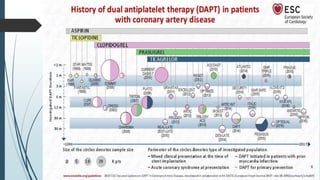
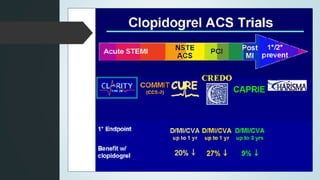
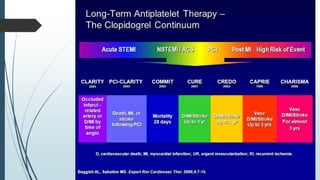
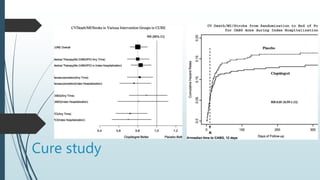
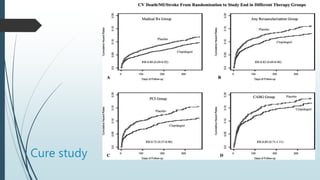
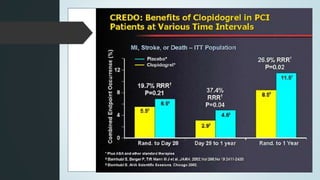
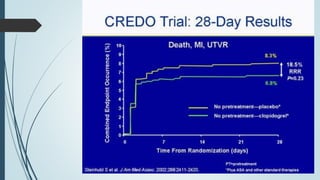
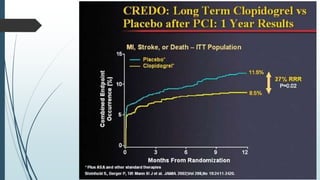
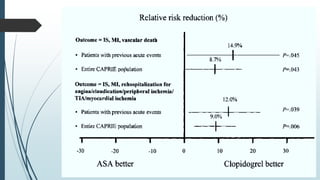
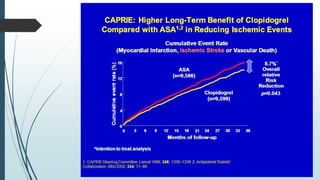
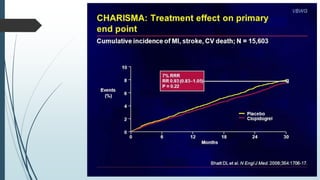

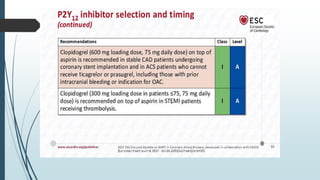
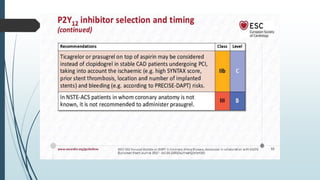
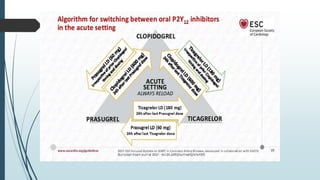
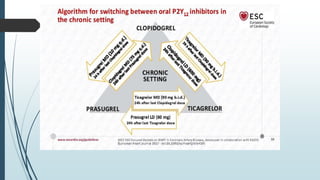
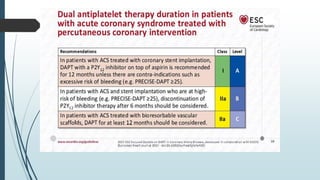
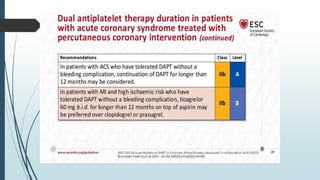
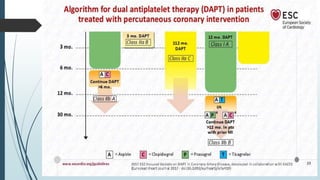
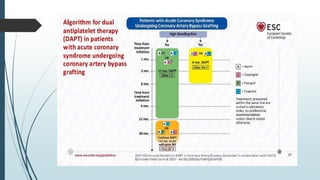
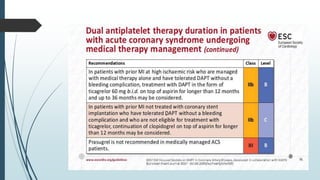


Clopidogrel is a pro-drug that requires hepatic metabolism to become active. It is a cornerstone of treatment for acute coronary syndrome (ACS) as dual antiplatelet therapy with aspirin. The CURE trial showed clopidogrel plus aspirin reduces cardiovascular events in ACS patients compared to aspirin alone. Later trials like CREDO found clopidogrel reduces events in patients post-percutaneous coronary intervention compared to aspirin. Newer P2Y12 inhibitors like prasugrel and ticagrelor are more effective at preventing ischemia but with increased bleeding risk. De-escalating dual antiplatelet therapy from newer drugs to clopidogrel appears safe and effective.





































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)

![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)











![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)



