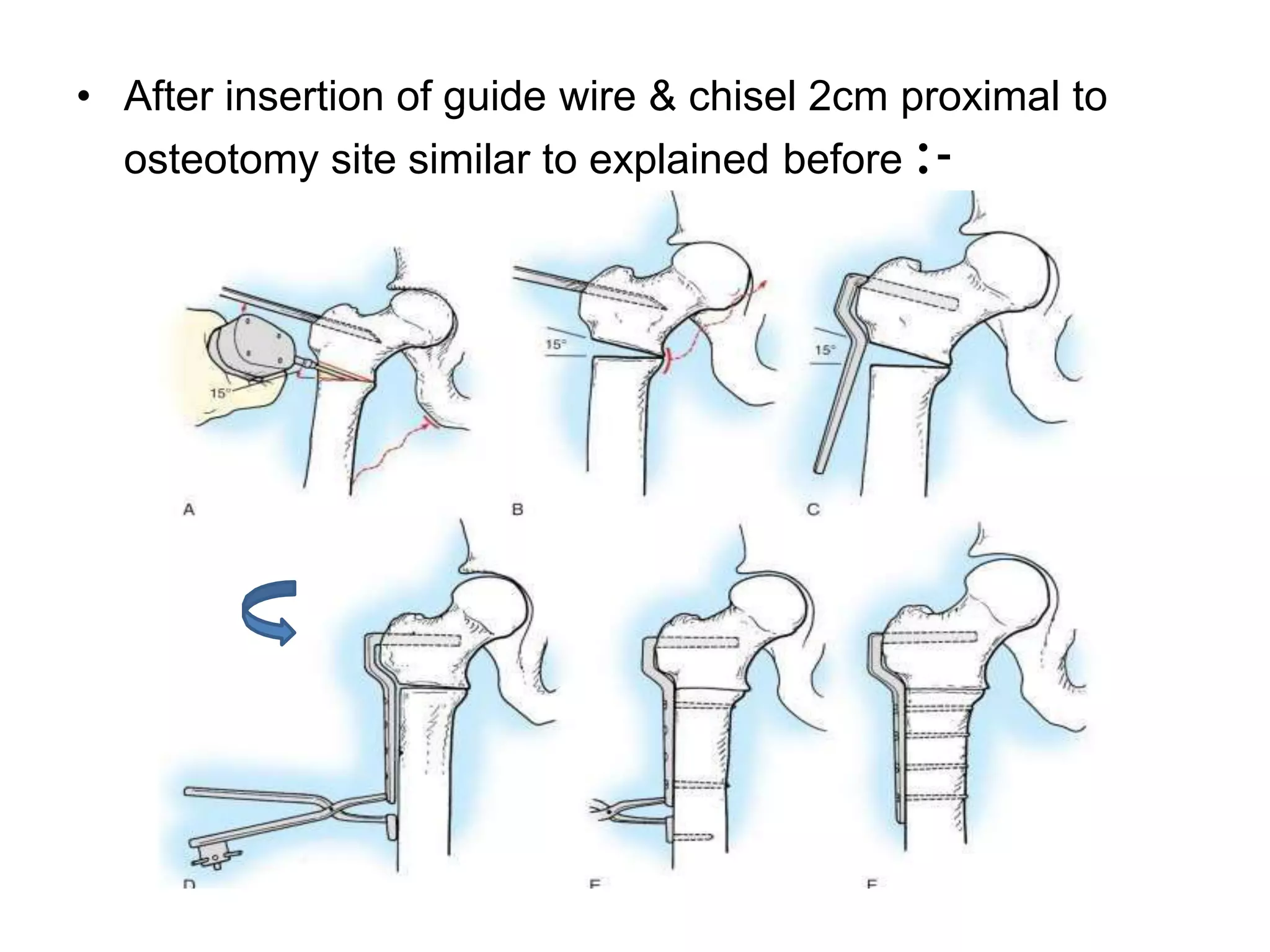
Proximal femoral osteotomies are surgical procedures used to correct biomechanical alignment of the lower extremity through removal of a portion of bone near the femur. The objectives include improving coverage of the femoral head, containing the head, moving normal cartilage into the weight bearing zone, improving motion, relieving pain, and correcting leg length inequality. Various types of proximal femoral osteotomies are classified based on anatomical location, degree of bone displacement, and surgical indications. Common indications include osteoarthritis, femoral neck fractures, slipped capital femoral epiphysis, Legg Calve Perthes disease, and congenital hip dislocations.