Downloaded 58 times





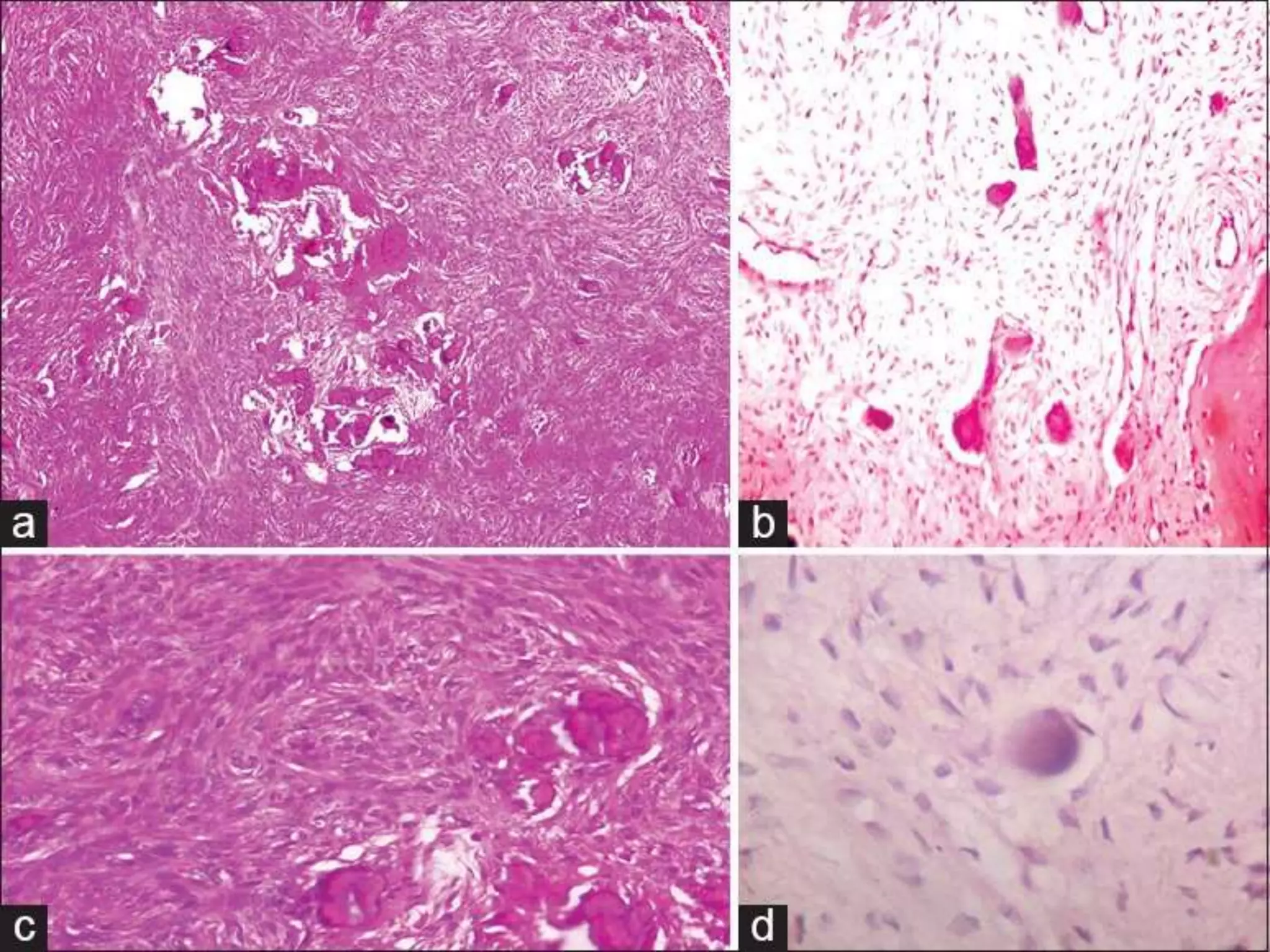
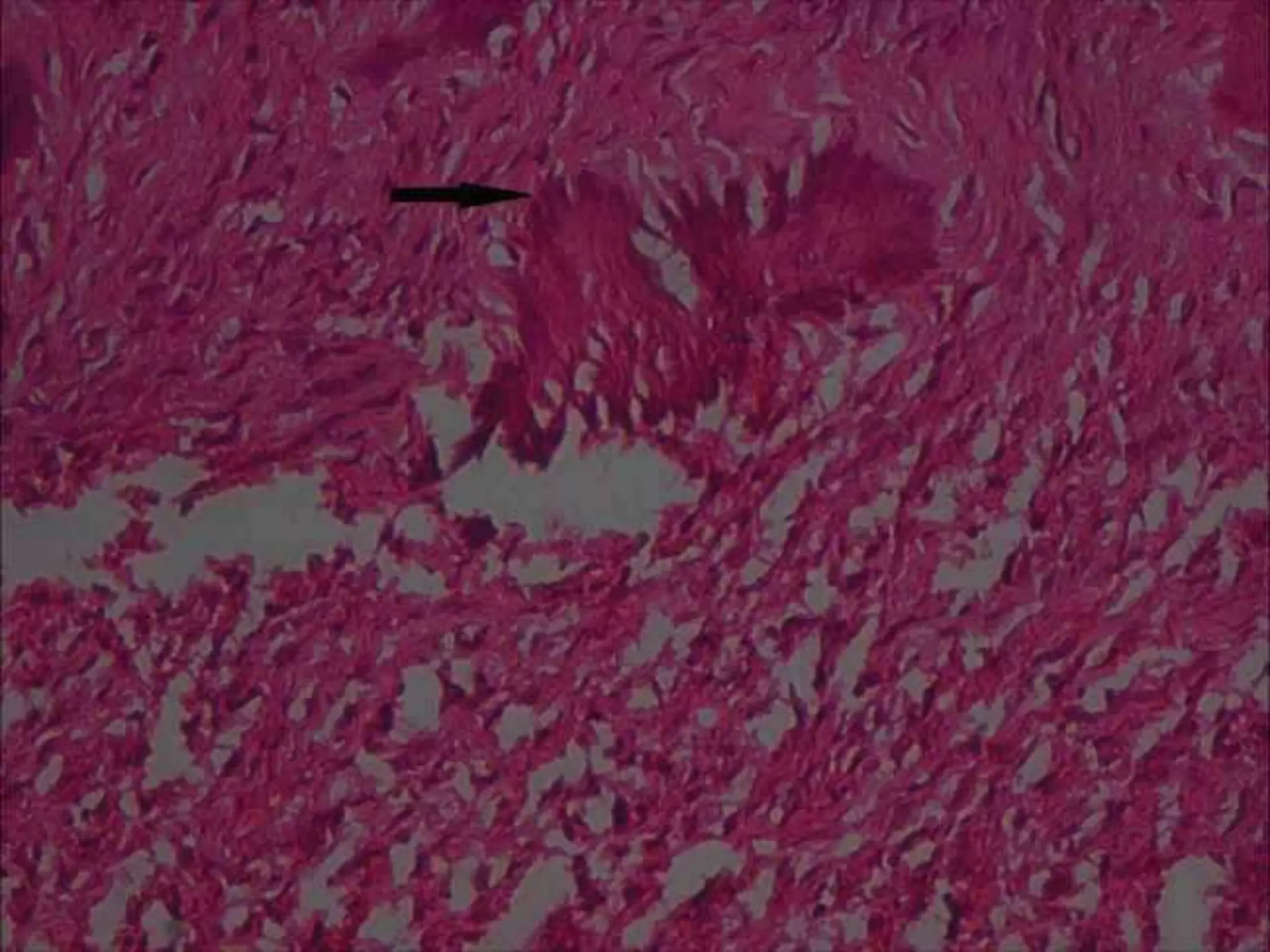
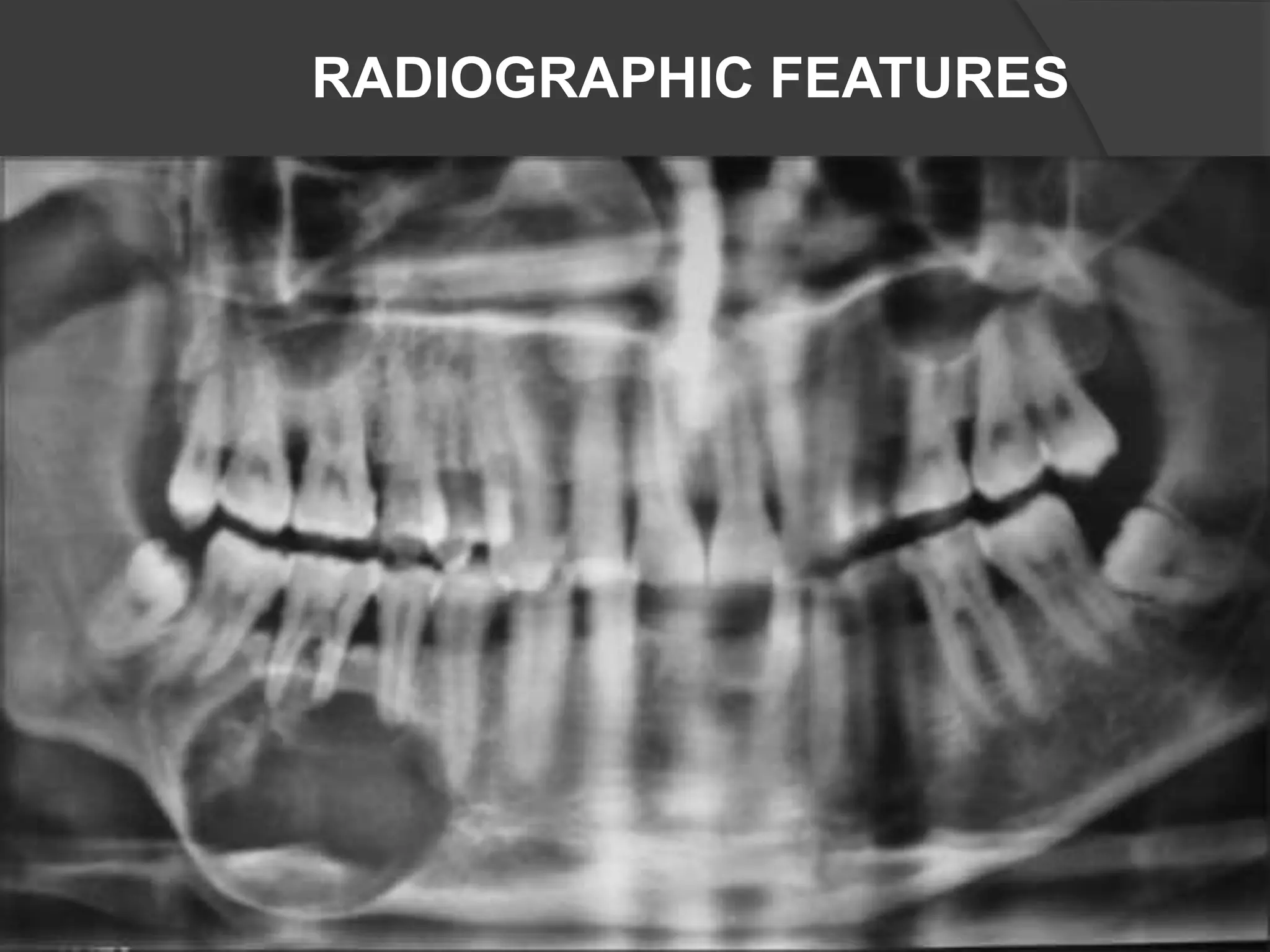
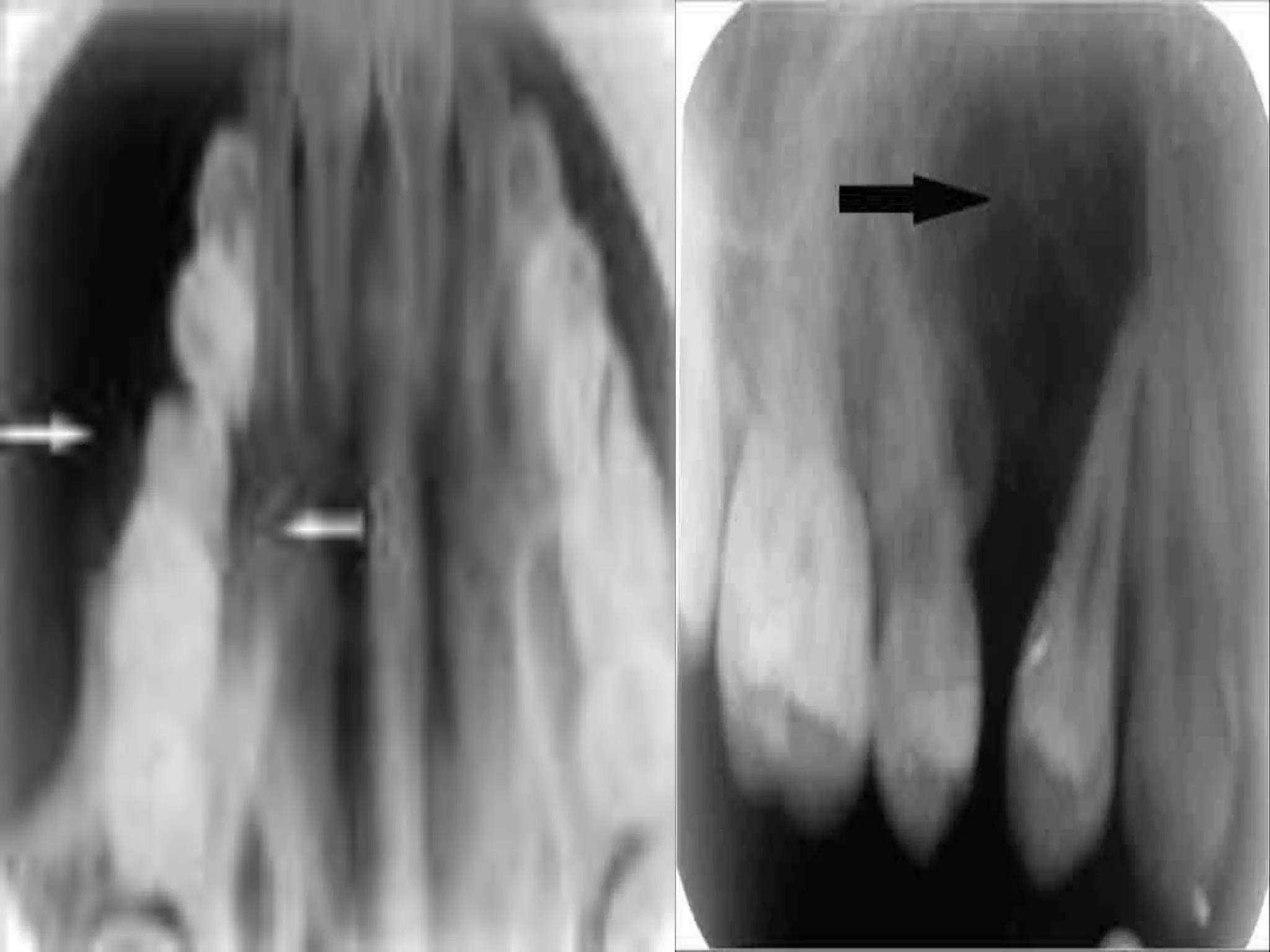
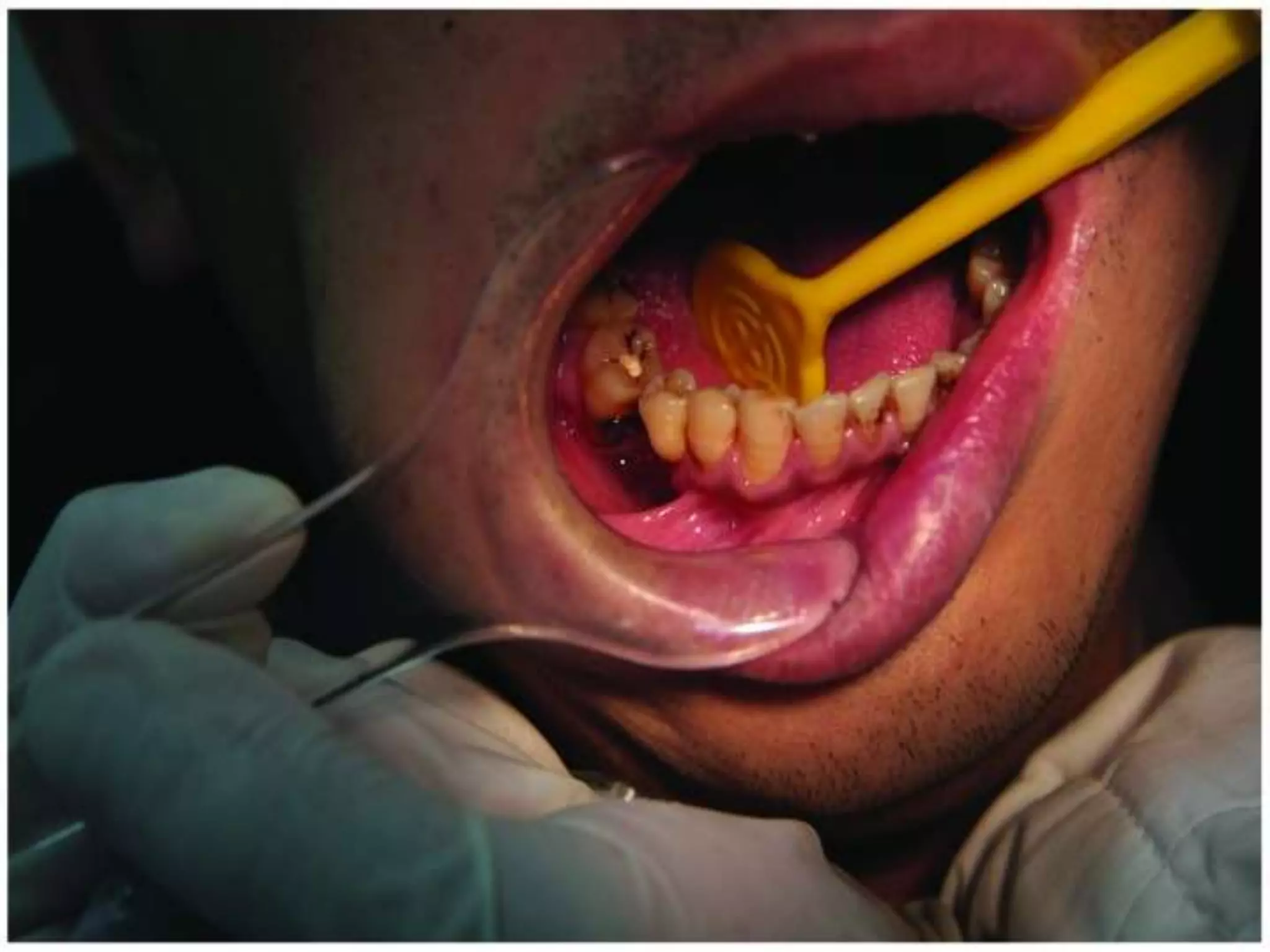
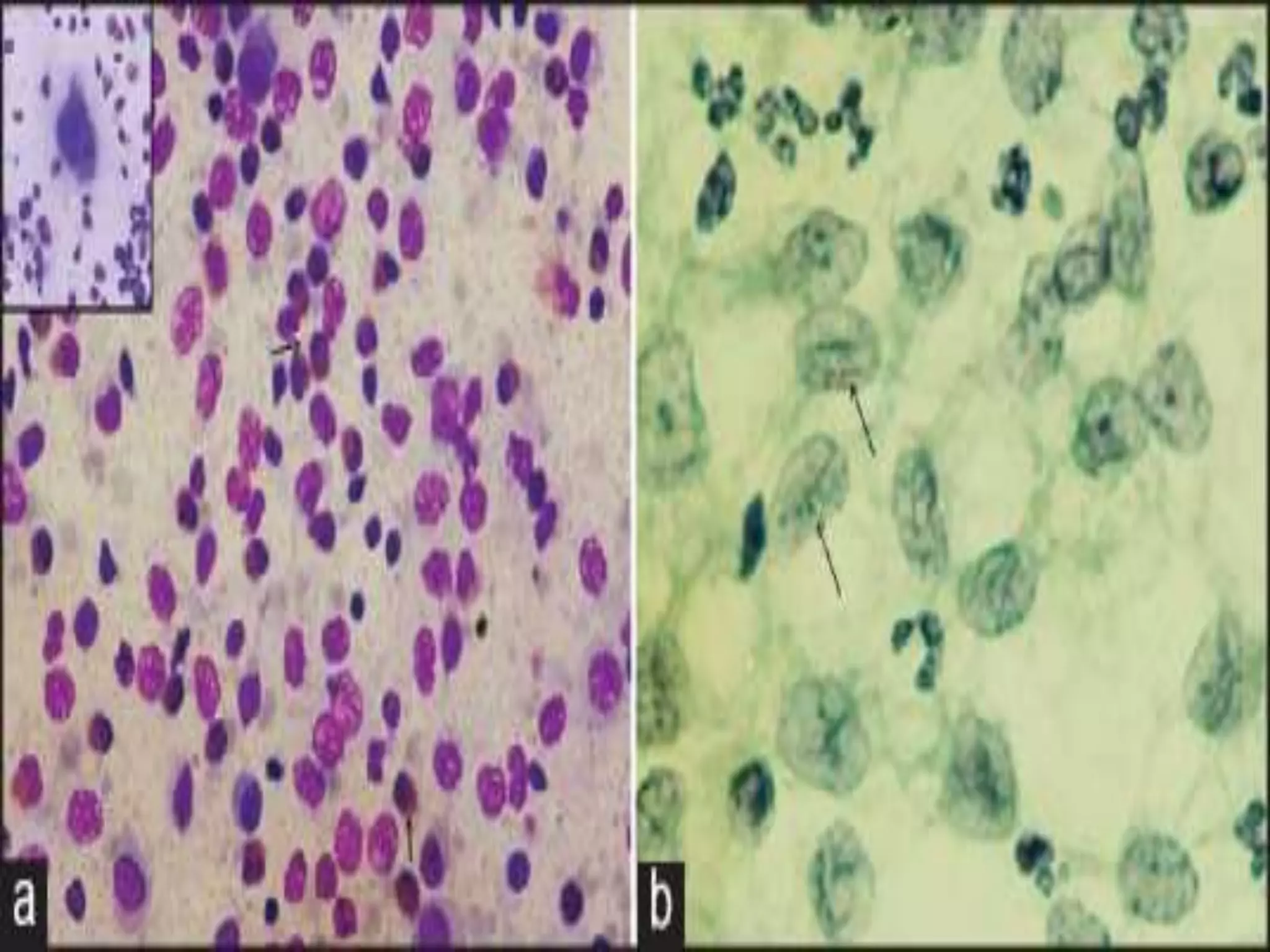
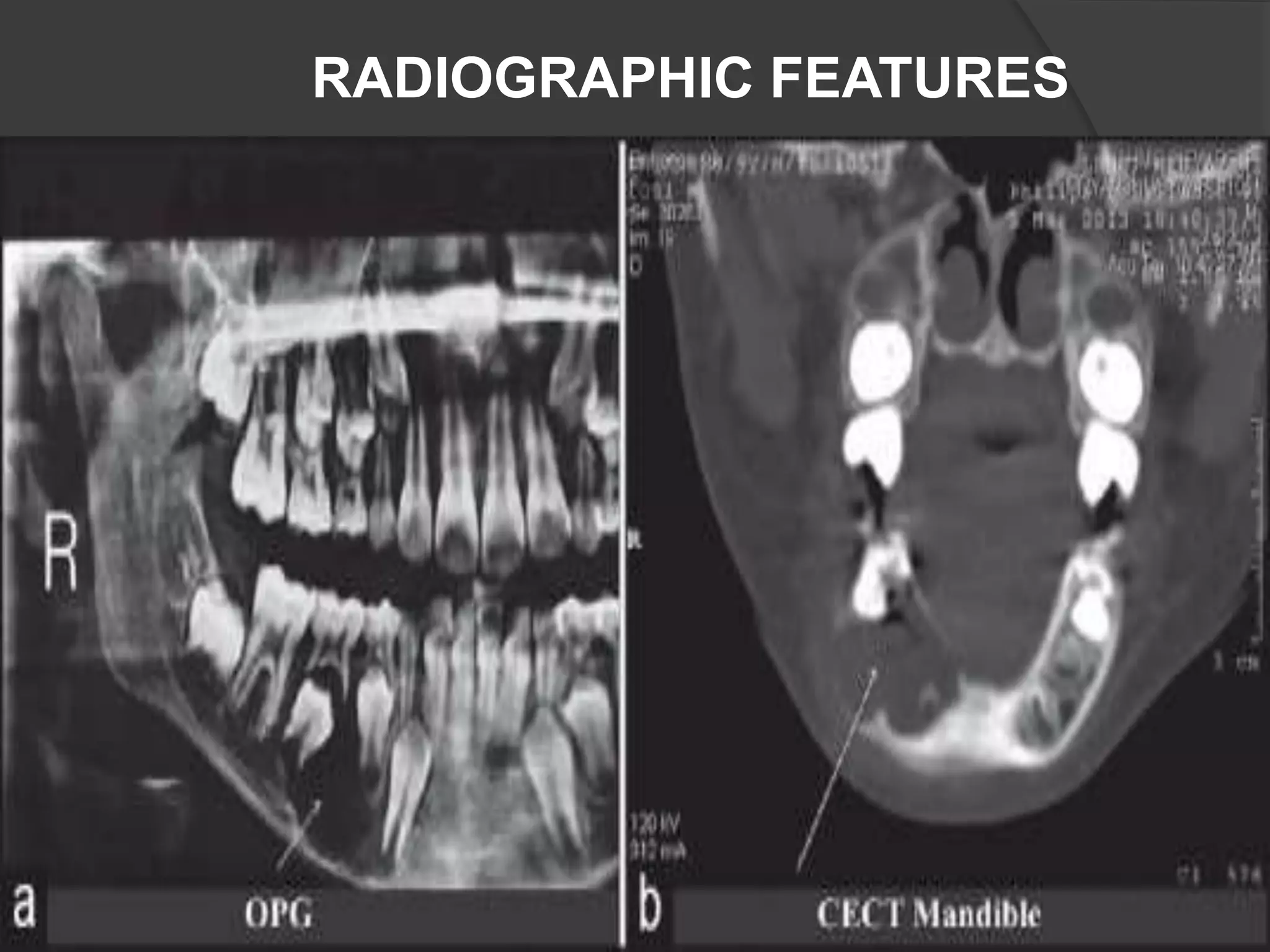
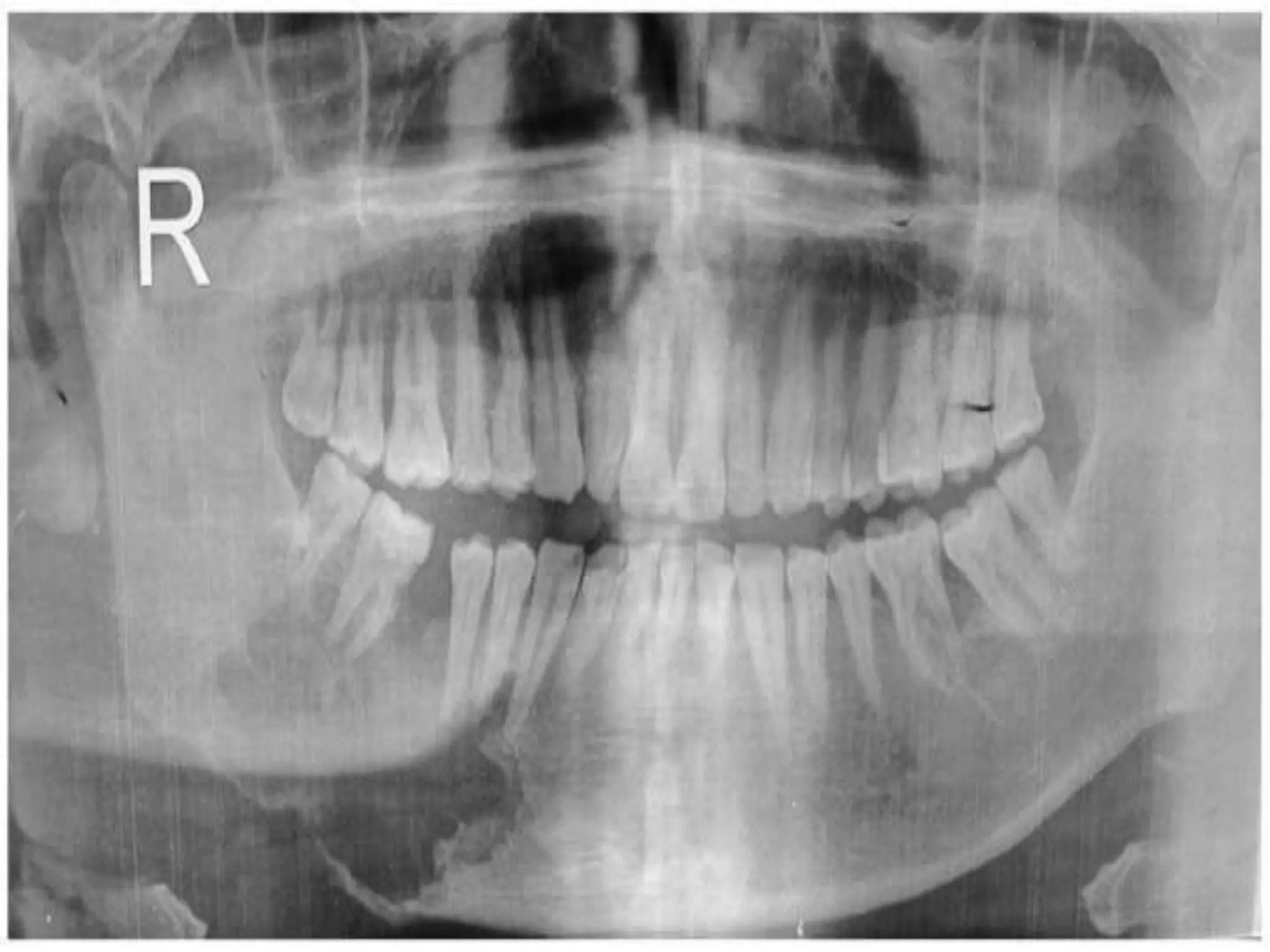



This document defines and describes several bone and jaw conditions, including osteoma, cemento-ossifying fibroma, and Langerhans cell histiocytosis. Osteoma is defined as a rare, benign bone tumor characterized by proliferation of compact or cancellous bone. Cemento-ossifying fibroma is a rare benign tumor of the jaw characterized by massive deposition of cementum and calcified material mixed with fibrous tissue. Langerhans cell histiocytosis is characterized by abnormal proliferation of immature dendritic cells and can present as eosinophilic granuloma, Letterer-Siwe disease, or Hand–Schuller-Christian syndrome depending on severity and site of involvement. Each condition is























































































