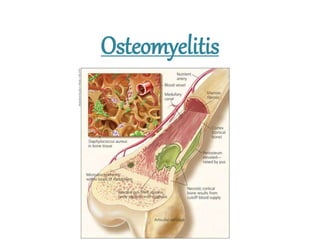
Osteomyelitis has been recognized since ancient times. It is an infection of bone that can be caused by bacteria, fungi, or other microbes entering through the bloodstream or directly through trauma. The most common type is acute hematogenous osteomyelitis, which typically affects children under 15 and presents as a rapidly destructive infection of the metaphysis of long bones. Staphylococcus aureus is the primary causative organism. Diagnosis involves blood tests, imaging like x-rays, ultrasound, bone scans or MRI, and tissue sampling. Treatment involves antibiotics along with surgical drainage and debridement if abscesses form or the infection fails to respond to antibiotics alone. Chronic osteomyelitis can develop if not properly