Download as PDF, PPTX
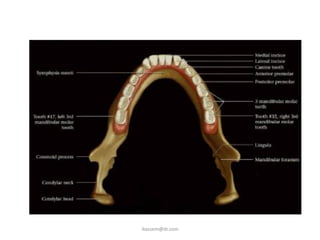
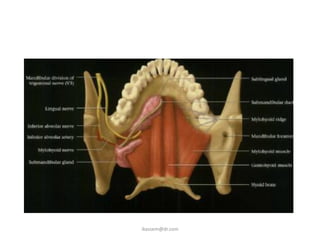
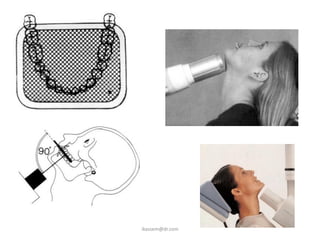
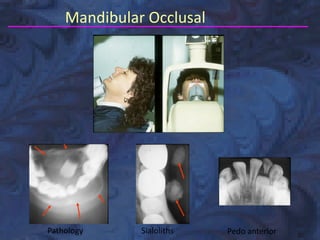
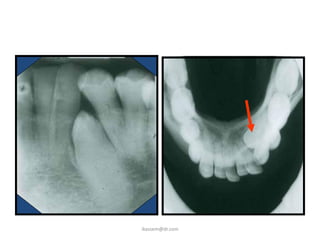
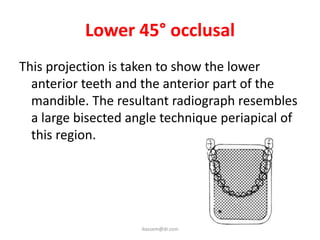
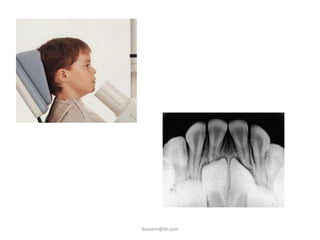
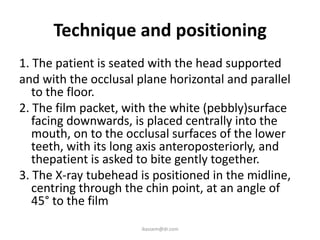
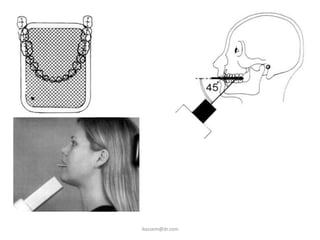
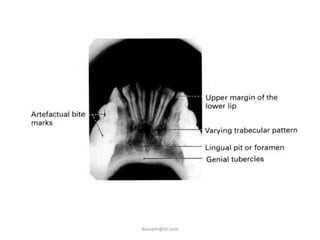
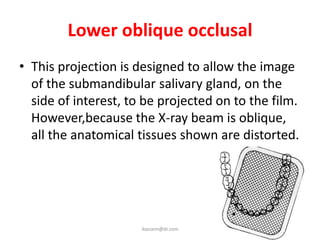
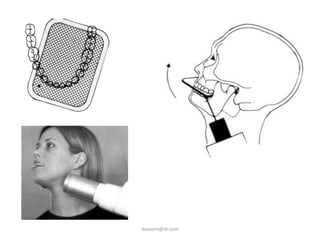
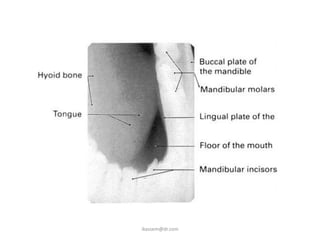


The document discusses various occlusal radiographic techniques for the mandible and maxilla. It defines occlusal radiography and describes the standard projections including upper and lower occlusal, oblique occlusal, and vertex occlusal views. The main clinical indications and techniques for the lower 90°, lower 45°, and lower oblique occlusal projections are outlined.