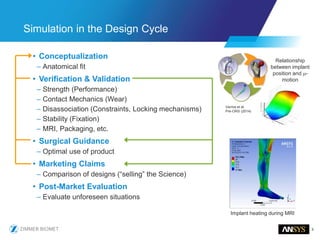
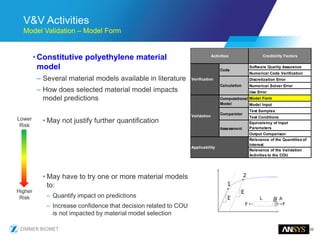
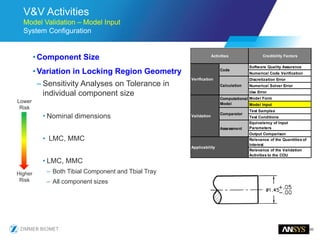
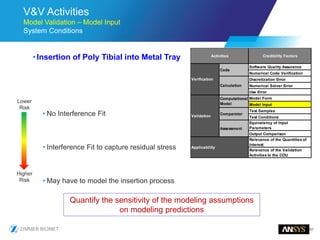
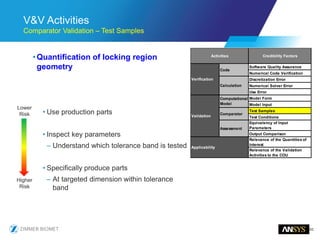
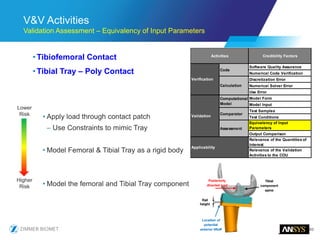
The document discusses the role of computational modeling and simulation (CM&S) in the total product lifecycle of orthopedic devices, emphasizing its use in device design, regulatory submission processes, and post-market evaluation. Key aspects include verification and validation (V&V) standards, the impact of regulatory frameworks, and how these models can predict device performance to improve safety and efficacy. Challenges and opportunities within the context of using CM&S for medical devices, including addressing uncertainties and leveraging real-world evidence, are also explored.














































![[Wroclaw #6] Medical device security](https://cdn.slidesharecdn.com/ss_thumbnails/medicaldevicesecurityowaspnopictures-170531065557-thumbnail.jpg?width=640&height=640&fit=bounds)














































