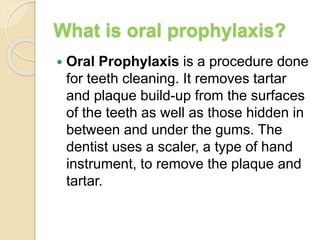
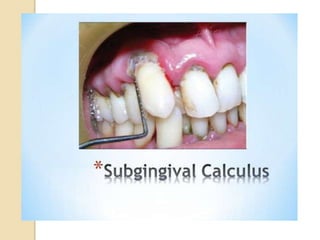
Oral prophylaxis, also known as teeth cleaning, is a dental procedure that removes plaque and tartar from tooth surfaces. It is generally performed using a scaler instrument to remove buildup above and below the gumline. Regular cleanings every 6 months are recommended for patients with good oral health to prevent periodontal disease. For patients with gum disease, a deeper cleaning called scaling and root planing is needed to remove tartar and bacteria from deep under the gums. The cleaning procedure involves removing supragingival and subgingival deposits using both hand instruments and ultrasonic scalers, followed by polishing, fluoride treatment, and home care instructions.