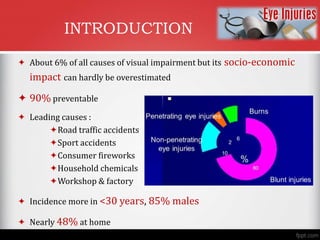
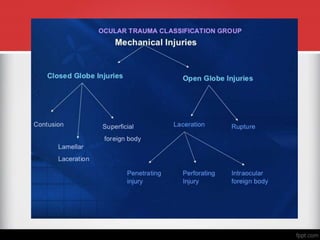
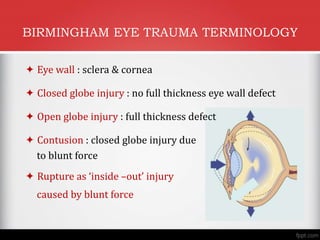
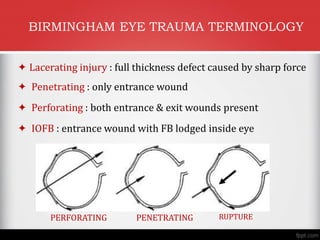
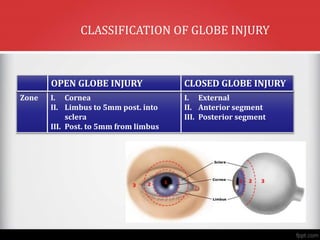
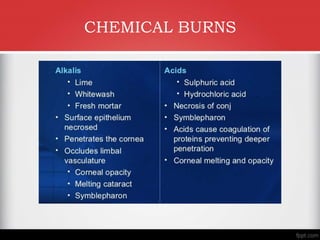
This document provides a classification and management protocol for ocular injuries. It begins with an introduction noting that ocular injuries account for 6% of visual impairment and are 90% preventable, with leading causes being road accidents, sports, fireworks and chemicals. It then covers objectives of classifying injuries, evaluating the injured eye, and emergency management. The document provides detailed classifications for types of ocular trauma (mechanical, chemical, thermal, combined) and terminology using the Birmingham Eye Trauma Terminology. It discusses evaluation, examination, imaging and emergency management of issues like chemical burns, open globe injuries, rise in intraocular pressure, and orbital hemorrhage. The key points are thorough evaluation and examination of the injured eye and