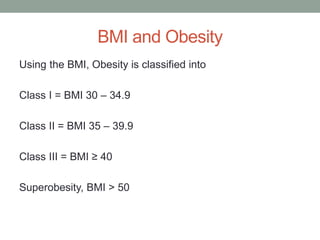
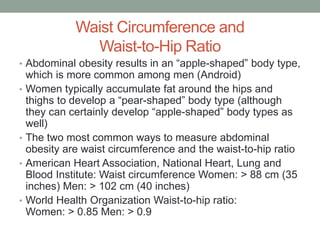
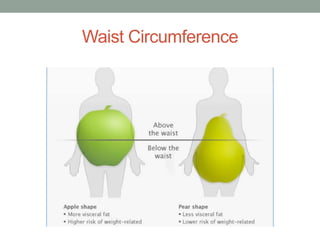
This document provides information on obesity, including its definition, causes, health risks, and treatment options. It defines obesity as a disease characterized by excessive body fat that increases the risk of health issues. The document discusses how obesity is measured using body mass index (BMI) and waist circumference. It outlines the genetic and environmental factors that contribute to obesity and explains how obesity increases inflammation and risk for conditions like diabetes, cancer, and heart disease. The document also reviews medical and surgical treatment options for obesity, including lifestyle changes, weight-loss medications, bariatric procedures like gastric bypass, and intragastric balloons.