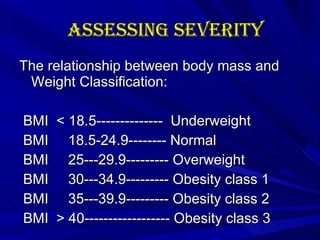
The document discusses the management of obesity through various means. It begins by defining obesity and assessing severity using body mass index (BMI) measurements. It then covers the etiology of obesity through factors like macronutrient properties, metabolism, hormones, and genetics. Various medical problems associated with obesity are outlined. Treatment options discussed include lifestyle changes, medications, and bariatric surgery. Criteria for surgical treatment and important preoperative preparations are also summarized.