Downloaded 57 times
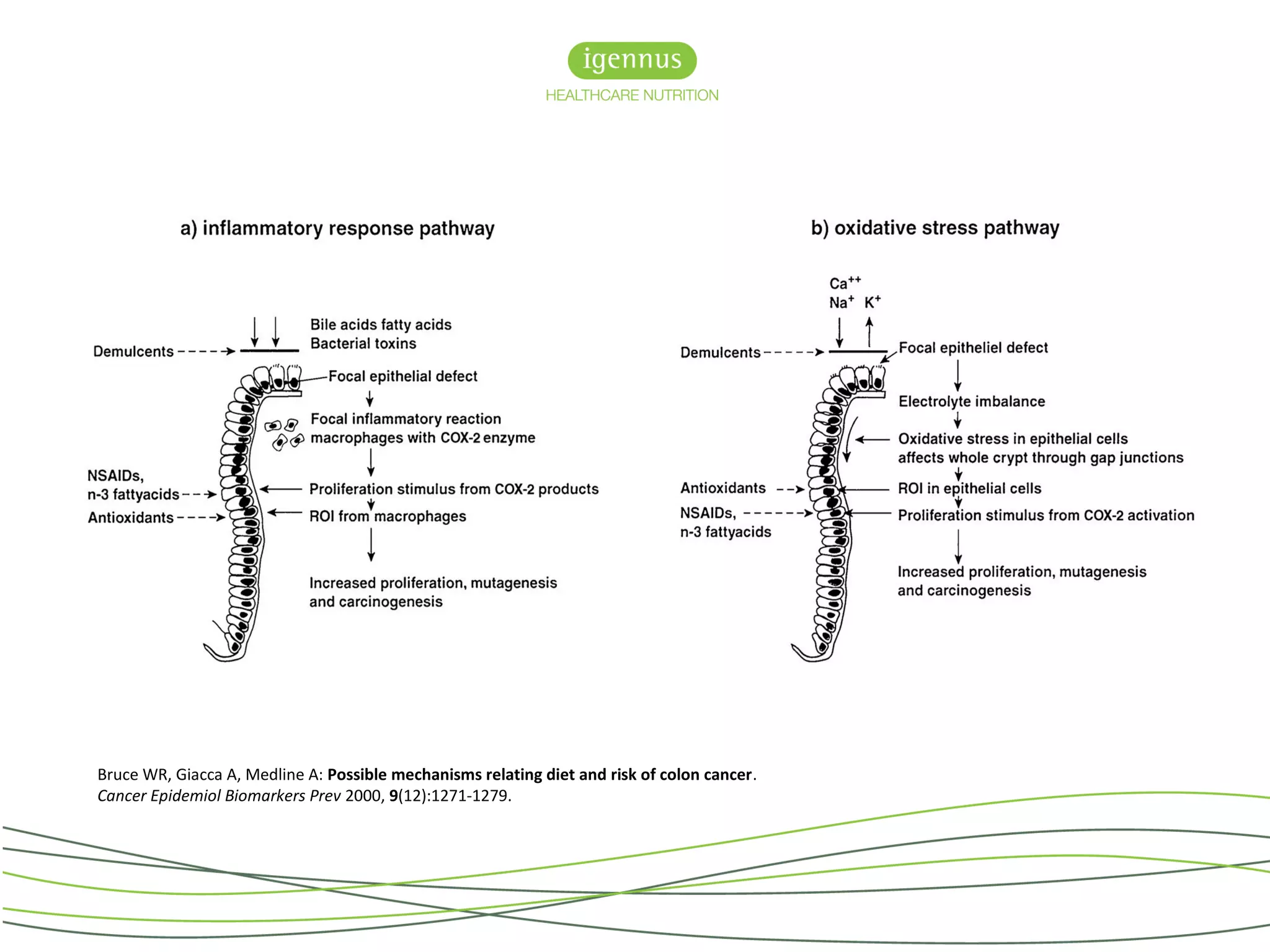
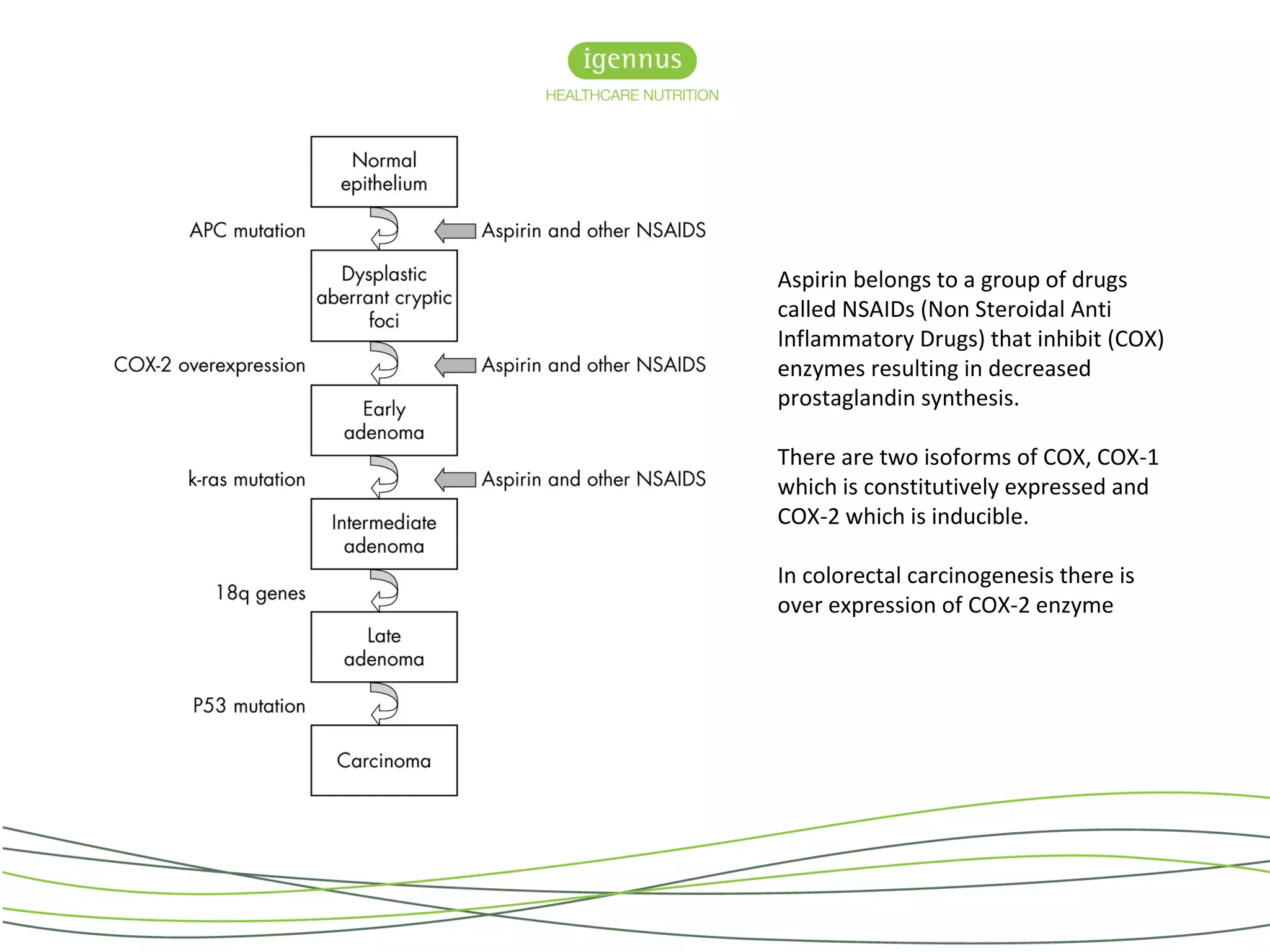


Colorectal cancer (CRC) is a major health issue in the UK, with a significant portion of cases potentially preventable through dietary and lifestyle changes. Diets high in omega-6 fatty acids are associated with increased CRC risk, while those rich in omega-3 fatty acids from fish may offer protective effects. The Seafood Polyp Prevention Trial aims to investigate the effectiveness of eicosapentaenoic acid (EPA), both alone and in combination with aspirin, in preventing colorectal adenomas in high-risk patients.































































































