Downloaded 170 times

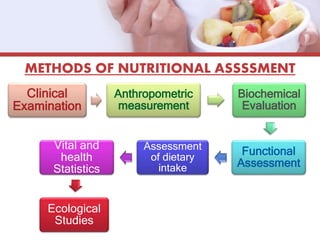

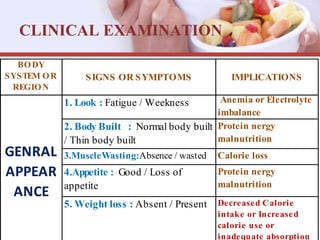
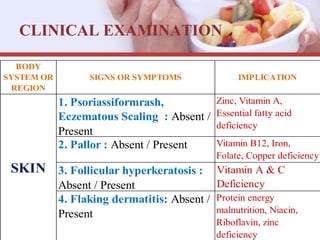
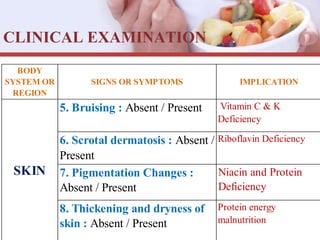
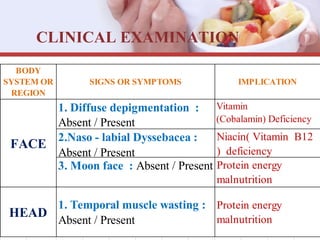
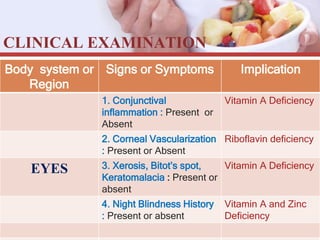


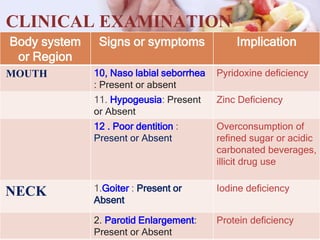

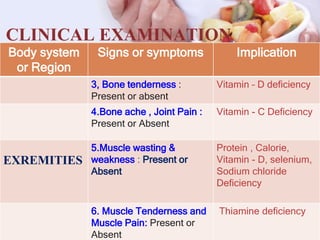

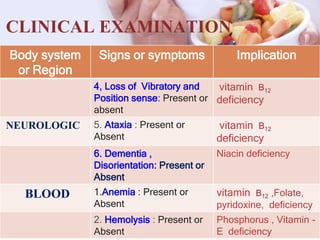

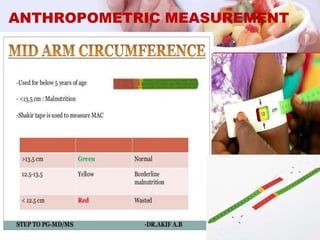

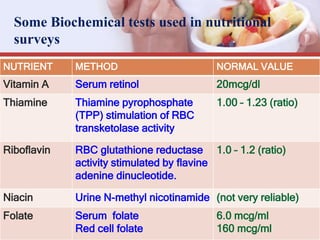
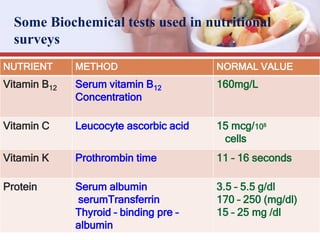
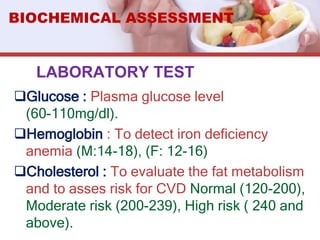


This document outlines various methods used for nutritional assessment, including clinical examination, anthropometric measurements, biochemical evaluation, dietary intake assessment, and analysis of vital statistics. Clinical examination involves a head-to-toe physical exam to detect signs of nutritional deficiencies. Anthropometric measurements provide objective data on height, weight, skin folds, and body mass index. Biochemical tests evaluate nutrient levels through blood and urine samples. Dietary intake is assessed through methods like 24-hour recalls, food frequency questionnaires, and food diaries. Vital statistics can identify at-risk groups and nutritional issues in a community.